
Bioinert ceramic biomaterials: advanced applications
Abstract:
First-generation, inert ceramics exhibit excellent mechanical strength, corrosion and wear resistance. This chapter reviews the fundamental properties that make alumina, zirconia, titania and pyrolytic carbon the materials of choice for the production of numerous load-bearing implants. The shortcomings of these materials, namely their relative brittleness and limited ability to be integrated with soft and hard tissues in vivo, are also discussed as a limiting factor for their clinical application.
7.1 Introduction
Ceramics are inorganic materials that are generally formed by a high-temperature synthesis process. They are comprised of non-directional ionic and covalent bonds, and are typically crystalline in nature (Bauer et al., 2013). The first generation of ceramics was hard, stabile and inert under a wide range of environmental conditions, often displaying superior properties to metallic biomaterials.
Metal-based alumina, zirconia and titania are amongst the most highly studied ceramics. The high compressive strength, low friction, corrosion and wear resistance of alumina, zirconia, titania and pyrolytic carbon makes these ceramics an excellent material for the fabrication of load-bearing implants. The high abrasive strength of these ceramics renders them highly suitable for use as bearing balls in artificial joints. When compared to metallic ball heads, ceramic heads lead to less long-term wear when used in conjunction with a polyethylene cup, reduce aseptic loosening, and therefore exhibit a reduced degree of osteolysis within the peri-implant space (Ihle et al., 2011). Despite these advantages, ceramics suffer from the disadvantage that they can be brittle (due to the nature of ionic bonds), which somewhat limits their use in clinical applications (Bauer et al., 2013). However, their excellent osteoconductive properties also make ceramics a coating of choice for the encapsulation of metallic load-bearing implants, such as titanium and stainless steel.
7.2 Hardness, high compressive strength and wear resistance of bioinert refractory polycrystalline compounds
Alumina (Al2O3) and zirconia (ZrO2) oxides represent two examples of the most widely used inert ceramics, with applications in the construction of orthopaedic joint replacement and load-bearing implants, for example prosthesis, implant coatings and dental implants. These are discussed in the following sections, together with leucite-containing ceramics.
7.2.1 Alumina
Alumina-based ceramics are typically prepared from very fine-grained polycrystalline α-Al2O3 using hot isostatic pressing, followed by sintering at temperatures of 1600 to 1800 °C. The compressive strength of alumina is notably higher than that of zirconia at 4250 and 2000 MPa for α-Al2O3 and tetragonal zirconia stabilised with yttria, respectively. The Young’s modulus and hardness for the former was greater, at 400 GPa and 2400 HV, respectively, compared to 208 GPa and 1130 HV. However, for zirconia, the bending strength was found to be higher for the zirconium oxide (1000 MPa) compared to 595 MPa for α-Al2O3. In comparison, the bending and compressive strengths of dense hydroxyapatite ceramics are 20 to 80 MPa and 100 to 900 MPa, respectively, with a Young’s modulus of 70 to 120 GPa and hardness of 500 to 800 HV.
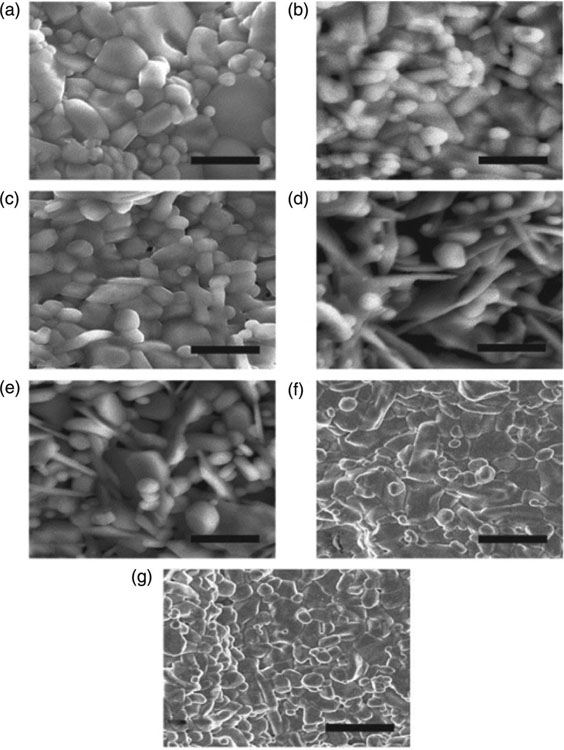
The mechanical properties, strength and corrosion resistance in crystalline materials is known to depend on the grain size within the material. Studies have demonstrated that for alumina to maintain its favourable mechanical and wear properties, the grain size should be kept below 4 μm, since an increase in the grain size to more than 7 μm has been shown to reduce the mechanical strength of the ceramic by close to 20% (Bauer et al., 2013). Addition of magnesium oxide to the α-Al2O3 facilitates the preservation of the fine-grained structure during the sintering process, contributing to the increased strength, resistance to dynamic and impact forces, fracture toughness and subcritical crack growth resistance. Figure 7.1 shows differences in microstructure and alumina doped with Ca, Mn and Cr (Pabbruwe et al. 2004). However, the use of such sintering agents should be kept to a minimum, since their excessive use may result in precipitation at the grain boundary and a consequent loss of fatigue resistance. In addition, implant materials that have a Young’s modulus that is relatively compared to that of natural bone tissue have been associated with aseptic loosening of the implant, with this behaviour being typically observed in metallic implants, such as those based on titanium.
Ceramics based on alumina are used in clinical applications such as dental bridges and implants, joint prosthesis, bone screws, alveolar ridge and maxillofacial reconstructions (Cruz-Pardos et al., 2012; Huet et al., 2011). Under load conditions that are typical for load-bearing applications (12 kN), alumina-based implants are expected to perform for 30 years, with their lifetime being limited by the material properties and the environment in which the ceramics are required to operate (Ritter et al., 1979). The fracture mechanics theory used to make this projection assumes that fatigue failure is controlled by the slow crack growth of pre-existing flaws in the structure when placed in biological environments. For example, the long-term strength of glass-infiltrated alumina- and various zirconia-ceramics for applications in an oral cavity environment differed significantly (Tinschert et al., 2007). The study found that under moist environmental conditions, the glass-infiltrated alumina- and some zirconia-ceramics have a high susceptibility to subcritical crack growth, while zirconia ceramics containing 0.25 wt% alumina oxide demonstrated the highest initial and most favourable long-term strength.
7.2.2 Zirconia
As with Al2O3 ceramics, zirconia is biocompatible, exhibiting good corrosion resistance under normal physiological conditions. As mentioned previously, zirconia has higher bending strength and fracture toughness compared to alumina, making it highly suitable for load-bearing implant applications. Furthermore, the stress shielding between the bone and the zirconia is reduced compared to that of alumina, owing to the notably lower tensile modulus of the former material. Monoclinic at room temperature, zirconia crystallises to form a tetragonal phase at temperatures between 1000 and 1170 °C. Subsequent heating to a temperature of 2370 °C causes the zirconia to transform from a tetragonal to cubic phase. During the sintering process, zirconia also undergoes a volumetric expansion of 3 to 5%. As the material cools, the mechanical stresses within the structure form. This mechanical stress has been linked to the formation of cracks in ceramics that are based on pure zirconia. Sintering agents may be introduced to stabilise the phases during these temperature changes. Introduction of magnesium oxide, calcium oxide and yttrium oxide results in the formation of a partially-stabilised zirconia microstructure, that is, it is comprised primarily of cubic zirconia with minor monoclinic and tetragonal zirconia precipitates. For example, incorporation of CuO into zirconia ceramics resulted in a significant reduction of friction in a sliding test against Al2O3 balls, with the coefficient of friction reducing from 0.8 to values between approximately 0.2 and 0.3 (Pasaribu et al., 2003). The flexural strength of partially-stabilised zirconia has been reported to be further affected by the fabrication methodology and the properties of the powders used (Adolfsson and Shen, 2012). The introduction of low amounts of Y2O3 (2–3 %mol) into a tetragonal zirconia polycrystal yields a ceramic structure with typical grain size of under 1 μm and narrow size distribution.
As a result of their superior mechanical properties arising from its high crystallinity, yttrium oxide stabilised tetragonal zirconia polycrystals are attractive candidates for various load-bearing dental applications (Crisp et al., 2012; Tarumi et al., 2012). However, the same degree of crystallinity renders yttria-stabilised tetragonal zirconia polycrystals highly opaque, which is undesirable for dental restoration from an aesthetic point of view. Clinically speaking, the stability of an yttria partially-stabilised tetragonal zirconia implant will be highly dependent on the adhesive bond strength that exists between the zirconia-based core and the resins used for dental restorations (Jevnikar et al., 2012). In contrast to silica-based ceramics, chemically-inert zirconia ceramics exhibit resistance to etching with acids, such as hydrofluoric acid and functionalisation. A host of methods have been trialled to establish a long-term bond with this substrate, including mechanical and chemical roughening of the surface to create micro-scale retention, for example particle abrasion, tailoring bonding cements, for example zinc-phosphate, composite resin, glass ionomer and resin-modified glass ionomer cements, and deposition of thin layers, such as alumina coatings.
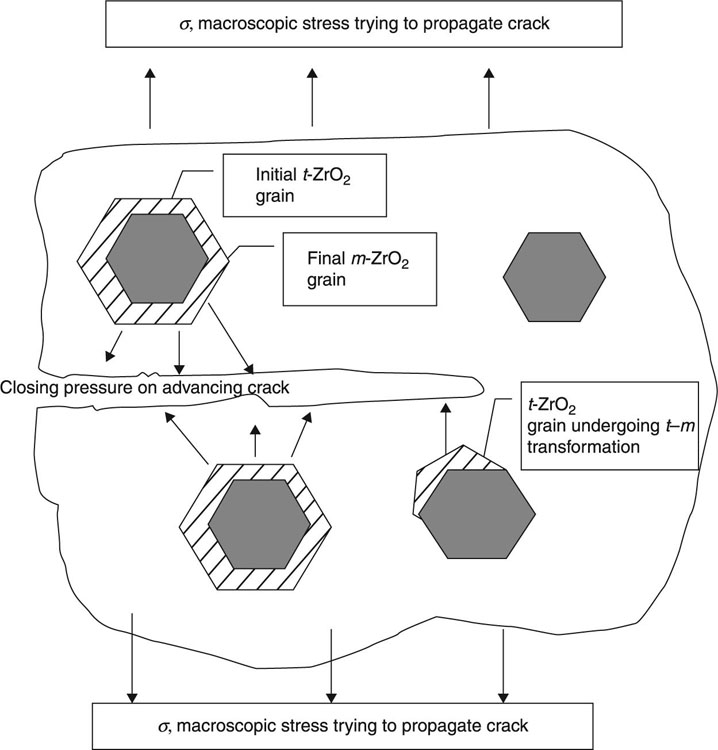
The addition allows for the stabilisation of the tetragonal phase at room temperature, with the size of the grain and the amount of yttrium oxide present affecting the proportion of the tetragonal phase retained. The retention of the metastable tetragonal phase is favourable, since it limits the extent of crack propagation. Specifically, the application of stress and resultant crack formation induces the metastable tetragonal zirconia grains located at the crack tip to transform to the stable monoclinic phase (Fig. 7.2). The expansion associated with the phase transformation works to offset the compression stress onto the materials, thus enhancing the mechanical roughness of the ceramics. In order to expand the desirable crack limiting characteristics of zirconia materials, these ceramic particles have been dispersed into the Al2O3 bulk ceramics to ensure mechanical pre-stressing of the resultant ceramics as the material loses its temperature after the sintering treatment. The resultant materials are characterised by a favourable flexing strength of over 900 MPa and a hardness of 1500 HV. However, it is not clear if the improvement in mechanical properties is associated with the microcrack formation. Furthermore, the wear resistance of alumina-containing zirconia particles has been shown to be less than that of pure Al2O3. In order to overcome this limitation, the zirconia particle size was reduced to a nanoscale.
Adding SrO and Cr2O3 to this nanoparticle zirconia-toughened alumina allows the formation of an alumina matrix composite ceramic (Bahraminasab et al., 2012). The mechanical properties of the composite are even more superior, exhibiting bending and compressive strengths of1150 and 4700 MPa, respectively, Young’s modulus of 350 GPa and hardness of 1975 HV. The enhanced mechanical strength allows for the development of more reliable, thinner walled components with a comparable load-bearing capacity. In orthopaedic applications, these materials could facilitate the fabrication of large ball heads to decrease the incidence of implant dislocation. In vivo studies using a sheep model showed a stable osseo-integration of porous coated alumina matrix composite ceramic monoblock cups (Schreiner et al., 2012). Clinical studies of the alumina matrix composite/alumina matrix composite-bearing surfaces showed no evidence of abnormal wear, osteolysis or implants migration (Lazennec et al., 2012).
7.2.3 Leucite
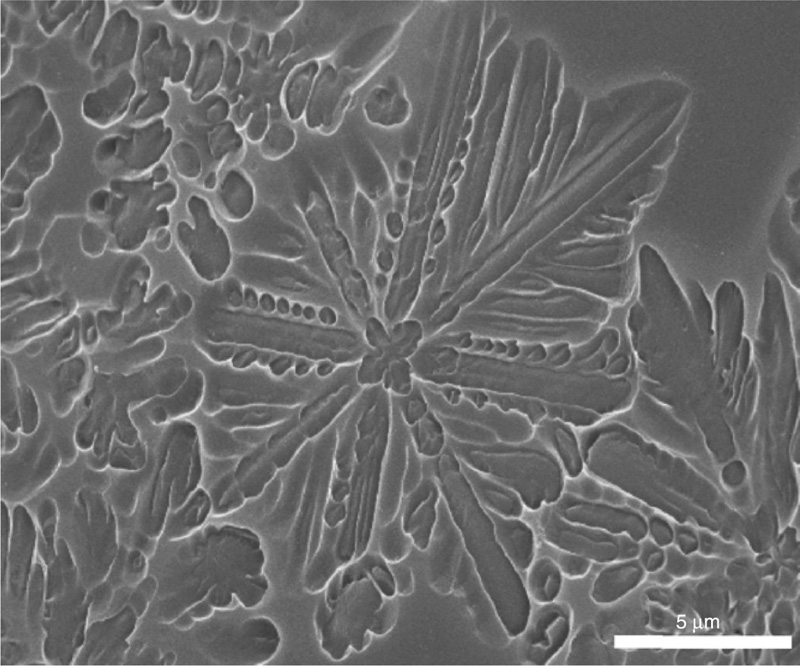
Leucite (KAlSi2O6) is a mineral composed of potassium and aluminium tectosilicate, with the crystals conforming to a polygonal shape and ranging in size from 1 to 5 micrometres (Fig. 7.3). At ambient temperatures, leucite crystallises to tetragonal structure, which is transformed to a cubic structure at 625 °C. A volumetric expansion of over 1% takes place during the displacive phase transformation, which is where a structural change is associated with the coordinated movement of atoms relative to their neighbouring atoms. Leucite is a major crystalline phase in ceramics that are used for dental veneers, termed feldspathic porcelains, where the amorphous phase is a feldspar-derived glass. Since the coefficient of thermal expansion of the glass phase is significantly lower than that of the underlying metallic implant, it is not suitable for veneering applications on its own. The incorporation of leucite notably increases the coefficient of thermal expansion. In terms of fabrication, leucite-containing ceramics can be prepared via the incongruent melting of naturally-occurring feldspars at temperatures between 1150 and 1530 °C (Bauer et al., 2013). As with other ceramics, microcracking within leucite-containing ceramics occurs as a result of the mismatch in the coefficient of thermal expansion between the crystalline and amorphous phases, causing a decoupling of crystals from the ceramic matrix. The thermal behaviour and the resultant mechanical properties and stability of leucite-based ceramics are dependent on the amount of the crystalline phase present. Typically, due to the presence of an extensive amorphous phase, leucite-based materials have been found to exhibit inferior mechanical properties compared to that of other biologically relevant inert ceramics.
7.3 Techniques for the fabrication of bioinert ceramic implants
The fabrication methodologies employed to manufacture finished implant products are vast, with the choice of method being dependent on the material and operation environment requirements. For instance, ceramic-based dental implants can be fabricated by heat pressing, slip casting, computer-aided hard machining of completely sintered ceramic units, or by sequential soft machining of partially sintered porous ceramic units and sintering (Denry and Holloway, 2010). Vacuum-aided sintering is commonly used for deposition of ceramic veneers, most commonly leucite-based feldspathic porcelains (15–25 vol% leucite) onto metallic dental implants. The technique is used to minimise the porosity of the ceramic veneer, as well as to reduce the presence of defects (cracks, inclusions) that may evolve into microcracks under operating pressure. Within the porcelain, the leucite particles have been shown to be partially encircled by the microcracks formed as a result of a thermal expansion mismatch between the leucite crystalline phase and the surrounding glass matrix, with the magnitude of the stress at the particle-matrix interface independent of the leucite particle size (Mackert et al., 2001). The firing/cooling cycles have been reported to influence the leucite concentration within the ceramic veneer, thus affecting the mechanical properties of the product. Slow cooling has been demonstrated to increase the proportion of crystalline leucite within the porcelain (Mackert and Evans, 1991). The ratio of crystalline leucite to amorphous feldspar glass affects the coefficient of thermal expansion of the resultant ceramic, and is fine-tuned to ensure that the thermal contraction of the veneer is less than that of the underlying metal unit (Mackert and Williams, 1996). In addition to tempering, ion-exchange treatments of feldspathic porcelains (via application of ion exchanging agents to the porcelain surface) have been demonstrated to create a surface less prone to crack initiation (Anusavice et al., 1992).
Heat pressing is an easy and inexpensive technique that has mostly been used to produce ceramics based on leucite and lithium disilicate with a reinforcing crystalline phase. The ceramics produced in this fashion contain a significantly higher proportion of crystalline component (35–45 vol% leucite), resulting in an enhanced bending strength and fracture toughness compared to that of veneers (Denry and Holloway, 2010). The observed improvement in the mechanical performance of heat pressed ceramics can be partially attributed to the dispersion of fine leucite crystals throughout the ceramic matrix and the difference in tangential compressive stresses around the crystal phase as a consequence of cooling. According to Guazzato et al. (2004), the highly localised residual stresses can arise in a region with thermal expansion anisotropy in polycrystalline materials with elongated grains and/or thermal expansion or elastic mismatch in polyphase materials and/or in transforming materials. These residual stresses induce the microcrack toughening of the material, where microcracks emerge along the lowest energy path, such as the lower modulus and toughness glassy phase in a glass-ceramic. However, the negative aspect of the microcrack evolution is the potential decoupling of the crystalline phase from the porcelain matrix, which can result in an untimely loss of strength and facture resistance.
While the typical porosity of heat pressed leucite-based ceramics is approximately 10%, a significantly lower porosity (~ 1%) can be attained using lithium disilicate (Li2Si2O5)-based ceramics (65 vol%). The heat pressing-induced crystallisation of lithium disilicate yields a highly interlocked crystal phase with nanosized dimensions, with lithium metasilicate (Li2SiO3) and cristobalite (SiO2) intermediates forming prior to the formation of lithium disilicate crystals. As with leucite-based ceramics, the formation of tangential compressive stresses at the boundary between Li2Si2O5 crystals and surrounding amorphous phase is associated with improved crack deflection and mechanical stability (Borom et al., 1975). The high proportion of the Li2Si2O5 to glassy phase and applied heat and pressure lead to crystal alignment, with the mechanical fracture toughness anisotropy. Specifically, the susceptibility to crack formation and propagation is significantly reduced in the direction perpendicular to crystal alignment.
As with other processes, the addition of a sintering aid into the ceramics precursor allows for property tunability of the resultant material. For example, hot pressing was used to produce fully dense ceramics from magnesium aluminate spinel (MgAl2O4) with a good optical transparency (> 80% throughout the visible spectrum). The determining parameter in attaining the high transparency was the addition of 0.25 wt% LiF agent prior to hot pressing at 1600 °C under vacuum and 20 MPa uni-axial load, followed by hot isostatic pressing at 1850 °C under 200 MPa Ar atmosphere (Sutorik et al., 2012). Other variables that affect the transparency of the resultant MgAl2O4 ceramics include heating rate, temperature, powder treatment and pressure at which the processing takes place. Recently, spark plasma sintering has been suggested as a good method for the production of transparent MgAl2O4 ceramics, which was found to be a superior technique compared to both hot pressing and hot isostatic pressing methodologies (Fu et al., 2013). Within a few minutes, the technique promises to achieve an almost full densification, resulting in a restricted grain growth and uniform grain-size distribution compared to that obtained using hot pressing.
Another approach used to produce dense ceramics is sequential dry pressing and sintering, where an over-sized specimen (10–20% larger than the final implant) is first fabricated using a computer-designed die and then sintered at a temperature of about 1550 °C. This production method is commonly used on high purity Al2O3-based ceramics and results in a high degree of crystallinity and a small distribution of grain size around a mean of 4 μm, the bending strength of approximately 600 MPa, and good in vivo stability for many years of use. Since the high crystallinity of the bulk material renders it opaque and not aesthetically pleasing for dental applications, the resultant product often undergoes finishing coating using a translucent porcelain veneer. The methodology is also suitable for fabrication of fine stabilised zirconia powders (Laberty-Robert et al., 2003). Uniaxial dry pressing and sintering (1400–1550 °C, 2 hrs) of yttria partially stabilised tetragonal zirconia yielded ceramics with a mean grain size of 0.26 to 0.57 μm (Kosma![]() and Kocjan, 2012). The temperature at which sintering took place affected the ageing characteristics of different ceramics. Furthermore, the properties of the powdered precursors had the greatest effect on ageing when sintered at lower temperatures, and minimal effect at higher sintering temperatures. Important powder characteristics include their ability to flow freely into the die and be packed with a minimal gradient; these will depend on the size and distribution of ceramic particles within the powder, their granular conformation (size, shape, distribution), the deformation that these granules undergo during pressing, etc.
and Kocjan, 2012). The temperature at which sintering took place affected the ageing characteristics of different ceramics. Furthermore, the properties of the powdered precursors had the greatest effect on ageing when sintered at lower temperatures, and minimal effect at higher sintering temperatures. Important powder characteristics include their ability to flow freely into the die and be packed with a minimal gradient; these will depend on the size and distribution of ceramic particles within the powder, their granular conformation (size, shape, distribution), the deformation that these granules undergo during pressing, etc.
For the fabrication of glass-infiltrated ceramics of spinel (MgAl2O4), alumina and ceria-stabilised ZrO2/Al2O3 nanocomposite, a process involving slip-casting, sintering and infilling is used (Bajpai and Bhargava, 2012; Della Bona et al., 2008). Slip-casting is first used to produce a highly porous three-dimensional structure from the aforementioned crystalline materials, which are then sintered at the temperatures appropriate for the chosen crystalline phase to produce a highly stable crystalline network. Then a lanthanum-based glass is introduced into the structure to produce the glassy phase network (Yang et al., 2012b). Sandblasting can be used to remove any excess glass. For Al2O3-based ceramics, the glassy phase represents approximately 27% of the material by volume at 5% porosity. The crystalline phase is composed of grains with wide size and shape distribution.
As with previously discussed ceramics, the difference in the coefficient of thermal expansion between the crystalline and glassy phases accounts for the microcrack formation and bridging, thus enhancing the mechanical properties of the material. Among the glass-infiltrated ceramics, MgAl2O4 has superior translucidity compared to Al2O3-based ceramics; however, the strength and fracture resistance is higher in the former material (Sutorik et al., 2012). Glass-infiltrated ceria-stabilised ZrO2/Al2O3 structures consist of 34 vol% Al2O3, 33 vol% of ceria-stabilised ZrO2 and 23 vol% glass phase, with a resultant porosity of approximately 8 vol%. The use of two different crystalline phases improves the mechanical toughness of the resultant ceramics, where zinc grains contribute to microcrack nucleation (due to compressive and circumferential tensile stresses associated with zirconia grains) and alumina grains provide crack deflection, contact shielding and crack bridging.
Hard machining involves the computer-aided machining of fully sintered ceramics in order to produce implantable components. The process is associated with considerable tool wear and results in the abundance of surface defects that may compromise the in vivo stability and compatibility of the material. A range of ceramics are based on feldspar, leucite, sanidine (Na,KAlSi3O8), lithium disilicate, alumina and zirconia (Denry et al., 2001). However, soft machining uses partially crystallised ceramics that can be post-treated with glass-infiltration, sintering, hot pressing, etc. to attain final mechanical strength. The obvious benefit is the ease with which these ceramics can be machined. For example, partially crystallised lithium disilicate-based ceramics, containing both metasilicate (Li2SiO3) and disilicate (Li2Si2O5) crystals, are characterised by a lower strength of 130 MPa. Both soft and hard machining processes incur a notable amount of wastage of the ceramic material, and involve a ceramic preform containing a high degree of detail regarding the implant uniformity, compaction density and robustness to enable computer machining.
A number of additive production methodologies have been developed to fabricate complex ceramic structures in a more time and economically efficient manner and increase the accuracy with which the implant is manufactured. The methodologies are based on the availability of small modular elements that can be assembled quickly yet reliably. Stereolithography is a cost-effective method that involves laser polymerisation of an UV curable monomeric system followed by removal of organic particles (Chartier et al., 2002). Robocasting is another computer-aided design/computer-aided manufacturing process, where ceramic paste is deposited in a layer-by-layer sequence to build up core and fixed partial denture structures (Silva et al., 2011). Selective laser sintering is a type of solid freeform fabrication in which a ceramic part is generated in layers from powder using a computer-controlled laser/scanning apparatus and power feed system (Bourell et al., 1992). Three-dimensional printing allows for manufacture of tooling and functional prototype parts directly from computer models via the deposition of powdered material in layers and the selective binding of the powder by ‘ink-jet’ printing of a binder material (Özkol et al., 2012; Sachs et al., 1992).
7.4 Conclusion
Inert ceramics are characterised by a favourable combination of mechanical strength, corrosion and wear resistance, making them well suited for a wide range of load-bearing applications, most notably as integral components of artificial joints and in dentistry. Indeed, alumina ceramics are frequently used for the fabrication of femoral joint heads to be used in conjunction with an ultra-high density polyethylene acetabular liner in hip arthroplasty. From a mechanical wear point of view, a ceramic–ceramic pairing would be even more beneficial, since it would reduce the incidence of the aseptic loosening associated with polymer wear. However, limited in vivo soft and hard tissue integration of alumina and other bio-inert ceramics leads to loosening of all-ceramics-based acetabular sockets in the pelvic bone. Along with brittleness, such poor osseo-integration hinders the potentially beneficial clinical applications of these ceramics. To circumvent these issues, several bio-activation strategies have already been reported. Among them, sodium hydroxide treatment and surface immobilisation of biological agents have already been demonstrated to successfully improve cell adhesion, proliferation and secretion of osteocalcin in the absence of the deteriorating effect on the short- and long-term strength behaviour. However, more research into the surface modification of ceramics is required to ensure that sufficient levels of cement–bone interaction take place if these materials are to be used clinically. This has resulted in second- and third-generation ceramic materials, which are discussed in Chapter 8.