
1
Introduction to Brain–Computer Interface: Applications and Challenges
Jyoti R. Munavalli1*, Priya R. Sankpal1, Sumathi A.1 and Jayashree M. Oli2
1ECE, BNM Institute of Technology, Bangalore, India
2Amrita School of Engineering, ECE, Bengaluru, Amrita Vishwa Vidyapeetham, India
Abstract
Brain–Computer Interface (BCI) is a technology that facilitates the communication between the brain and the machine. It is a promising field that has lot of potential to be tapped for various applications. To begin with, this chapter explains the basics of the brain and its function. It describes the BCI technology and the steps: from signal acquisition to applications. The signal capturing is done through invasive and non-invasive methods. The features from the brain signals are extracted and classified using various advanced machine learning classification algorithms. BCI is extensively helpful for health-related problems but it also has applications in education, smart homes, security and many more. BCI has its own share of challenges that it has to overcome so that it could be beneficial in the future use. We discuss about all the issues like ethical, technical and legal. This chapter provides an overview on BCI through basics, applications, and challenges.
Keywords: Brain-Computer Interface, BCI technology, BCI applications, BCI challenges
1.1 Introduction
“A man sitting in a garden enjoying his regular walk. There are three devices that are in use in the garden; a drone, a wheelchair, and a laptop. Each of them is controlled by the man without using any remote controller. Yes, he is controlling them with his mind. This is one of the examples of brain-machine interface and we will be having numerous of them in the near future.”
In the past 20 years, the world has seen tremendous changes in the technology. Many technologies were invented that really affected the society for/in their well-being. We are witnessing new arenas like Artificial Intelligence, Virtual Reality, electronic health records, robotics, Data Science, and many more. All these have revolutionized the healthcare delivery system. Artificial Intelligence has paved its way in diagnosis, prediction of diseases through its advanced algorithms like machine learning and deep learning [1]. Virtual reality assists in treatment plans like phobias and neurological disorders [2]. EMR-based real time optimization has improved the efficiency of hospital systems and aid in decision making, again through technological intervention [3–7]. It has been observed that robotic assisted surgeries and the extent to which data science was utilized during pandemic are the big marking of technology in healthcare (Healthcare 4.0). With these technological interventions, Brain Computing Interface (BCI) is one among them.
In 1920, the first record to measure brain activity of human was by means of EEG but the device was very elementary. Later in 1970, research on BCI that was particularly for neuro-prosthetic, began at the University of California, Los Angeles, but it was in 1990s that these devices were actually implemented in humans.
A Brain–Computer Interface is also referred as Brain Machine Interface or Mind-Machine Interface. BCI is a computer-based system that acquires the signals based on the activities in the brain and analyzes and translates the neuronal information into commands that can control external environment (either hardware or software). It is an Artificial Intelligence system that identifies the patterns from the collected brain signals. The electrical signals that are generated during brain activities are used in interaction or change with the surroundings. It allows individuals that are not capable to talk and/or make use of their limbs for operating the assistive devices that help them in walking and handling and controlling the objects [8]. BCI is extensively used in Medicine and Healthcare [9].
This chapter presents the overview of BCI: its history and basics, the process details with hardware components, its applications and then finally the challenges faced while dealing with BCI. We begin with the description of functional areas of brain.
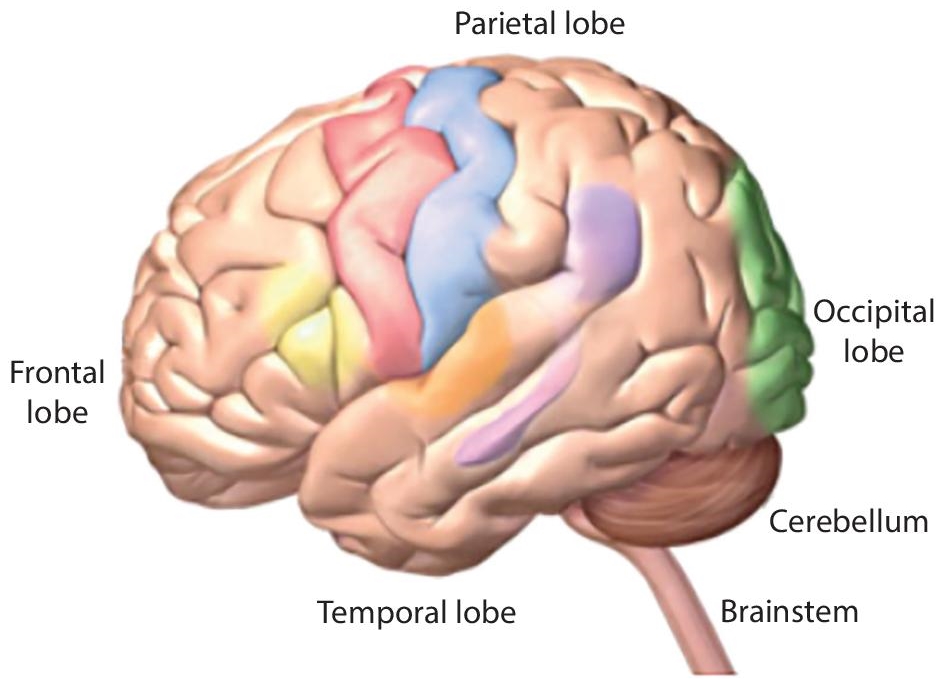
Figure 1.1 Brain parts.
1.2 The Brain – Its Functions
The brain is a soft mass made up of the nerves and tissues that are connected to the spinal cord. The main parts of the brain are Cerebrum, Cerebellum and Brain stem (see Figure 1.1). Frontal lobe, temporal lobe, parietal lobe and occipital lobe, are the four lobes of cerebrum. They are responsible for reading, learning, thinking, emotions, walking, vision, and hearing (regarding senses). Cerebellum is responsible for balancing and coordination. Brain stem is responsible for heartbeat, breathing, blood pressure, swallowing, and eye movements [10, 11].
Brain generates many signals and the electrical signals generated are used in BCI system. These signals are measured using invasive or non-invasive techniques.
1.3 BCI Technology
BCI as mentioned earlier is a communication channel between the brain and the external processing device. The goal of BCI technology is to give a communication model to those people who are severely paralyzed and do not have control over their muscles [12]. It takes the bio-signals measured from a person and predicts some abstract facet of cognitive state.
Most commonly, the BCI focuses on patients that have problems with motor state and cognitive state. In normal humans, there is an intersection of brain activity, eye movement, and body movements. If any one of them is missed, it results in constrained state. Figure 1.2 shows this intersection. It is observed that BCI is applicable to the areas where patients have normal to major cognition levels working along with no motor state response to minor motor state response. So under this umbrella, we get patients that experience completely locked-in syndrome (CLIS) or Locked-in Syndrome (LiS) [13].
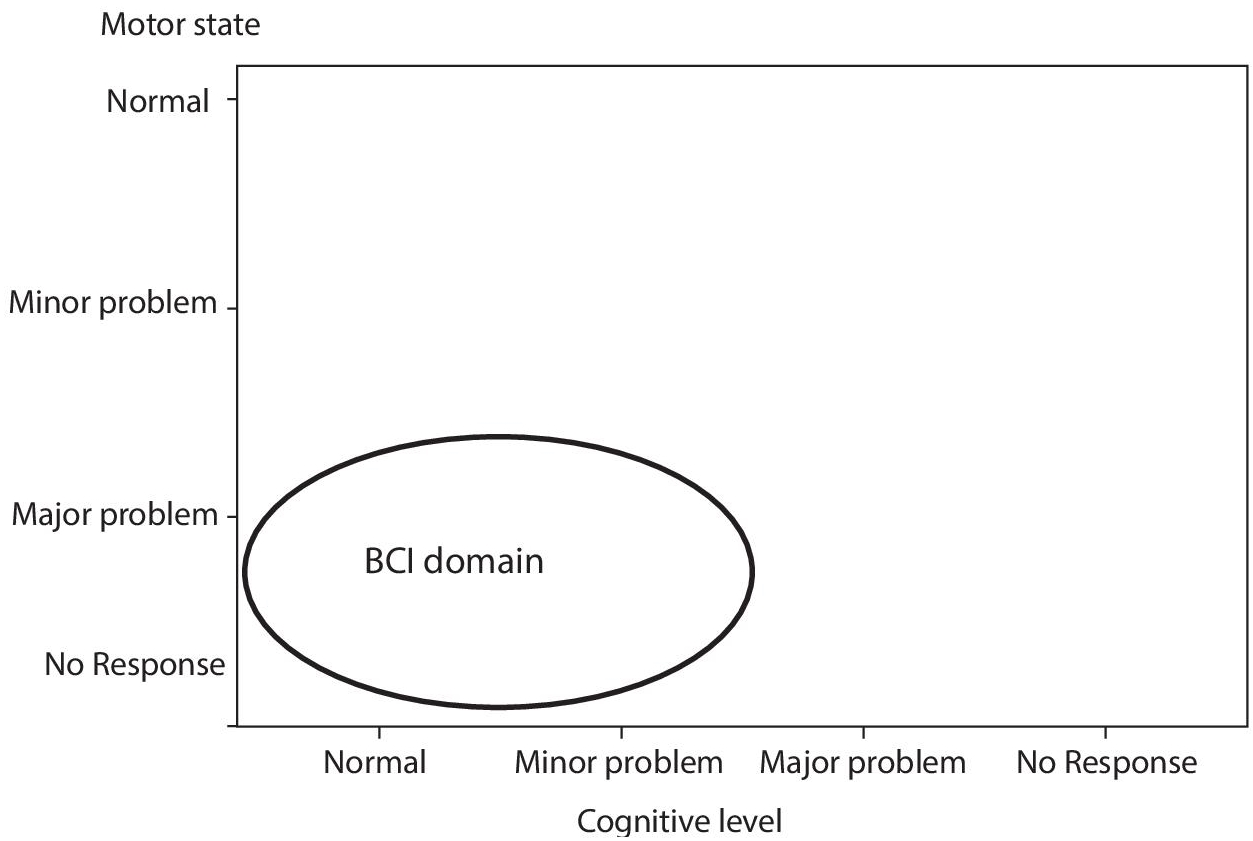
Figure 1.2 BCI domain.

Figure 1.3 Block diagram of BCI.
Locked-in syndrome is a neurological disorder also known as pseudo coma where patient is completely paralyzed that is losing control of voluntary muscles, except the eye movements. Therefore, such people can think and analyze but not speak and move. In recent past, it is seen that chronic LIS can be unlocked with the aid of BCI [14].
The block diagram of BCI is as in Figure 1.3. It begins with recording of signals from brain, then processing of these recorded signals. Here various features from the signals are extracted and classified as per their properties or characteristics. Based on these signals’ commands are generated and the BCI device works accordingly.
1.3.1 Signal Acquisition
In BCI, signal acquisitor plays an important role. There are different recording techniques in BCI and are broadly classified as invasive and non-invasive methods as shown in the Figure 1.4. These methods aid to bring out/pull out electric and magnetic signals of brain activity.
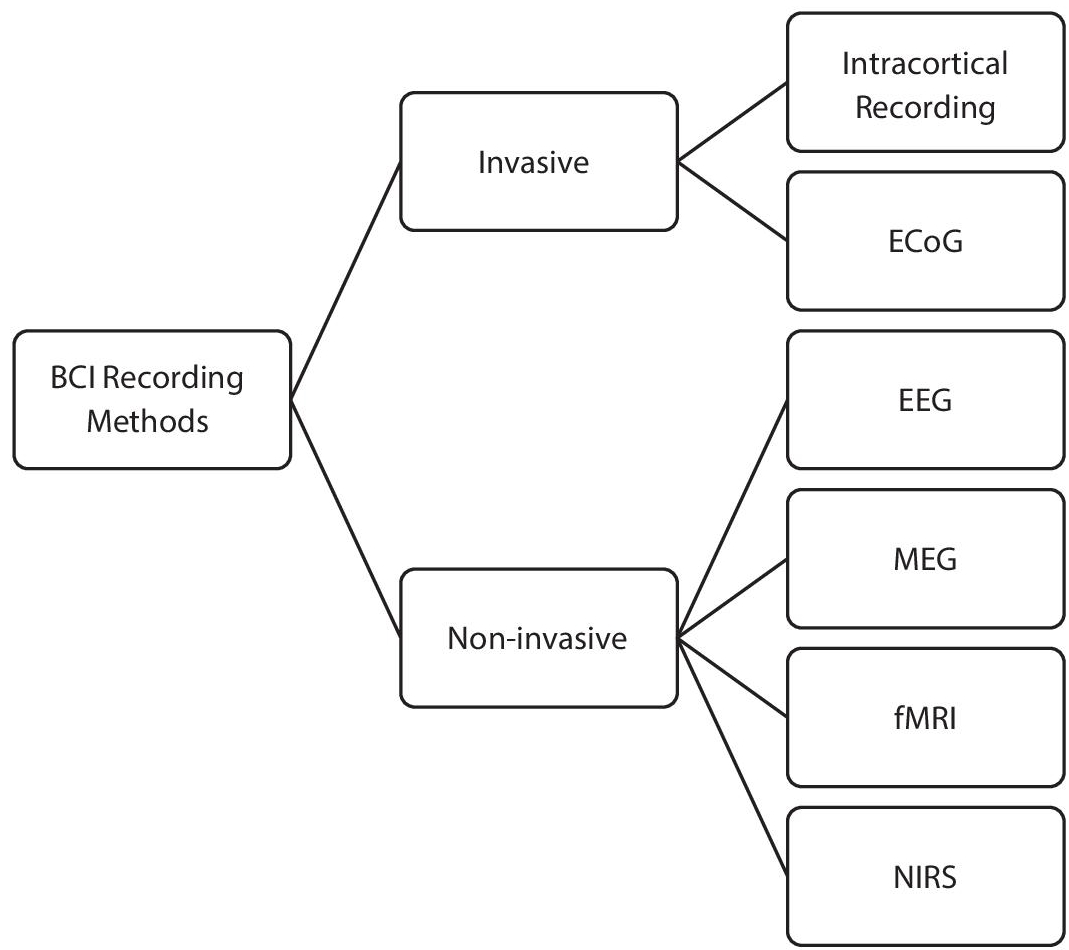
Figure 1.4 Types of BCI signal acquisitor.
1.3.1.1 Invasive Methods
Electrodes are implanted in the scalp to extract the required parameters and in non-invasive method, external sensors are used to measure the parameters.
a. Intra-Cortical Recording:
A single electrode or sometimes array of electrodes are in the cortex of the brain. These interfaces are been used for the past 70 years and some of the popular kinds of hardware for intracortical recording are as follows:
- Wire-based arrays
- Micro-machined micro-electrodes
- Polymer microelectrodes
i. Wire-Based Arrays
They are also called Microwire arrays, Wire arrays are made up of insulated metal wires with an uninsulated tip that is used to observe the bipotential form of neurons in a bipolar environment [15]. The diameter of those wires is in the range of 10–200 micrometers the limitations of microwire-based arrays are as follows:
- They are limited because of recording failures and FBR effects.
- Microwire arrays are highly prone to variation, disappearance, or disappearance of recorded signal in the timeframe spanning from weeks to months post-implantation [16].
- The wires are tedious to place and route to microelectronic packages.
- Isolation cracks, corrosion – analysis of tungsten microwaves extracted from rats after 9 months of use, revealed material deterioration in the form of isolation fractures and defamation.
- Extensive use of electrodes leads to electric leakages which result in errors when recording.
ii. Micro-Machined Micro-Electrodes
The introduction of photolithography and subsequent advancements in micromachining technology prompted the development of a new generation of silicon-based brain probes. (micromachined microelectrodes) [17]. Ex: Michigan Planar electrode arrays, Utah Electrode arrays [18].
The limitations are as follows:
- They degrade with time.
- Recording loss due to vascular mutilation.
- Failures in interconnection.
- Size and rigidity of the probes.
- Expensive (GoldPlatinum, Iridium are widely used in planar recording areas).
- They are prone to fracture.
- Failure in persistent recordings is mainly because of the 2D. geometry of MMEA-based reading electrodes.
- The size and mechanical mismatch of silicon-based and wire microelectrode arrays with the brain are two of the most important problems limiting the quality of neural recordings.
iii. Polymer Microelectrodes
The disadvantages of stiff materials can be potentially deviated using Polymers [19]. But they have certain limitations:
- The accuracy and depth of implantation of soft and flexible implants into the brain is hampered, making them difficult to implant [20].
- Complicated structural design.
- Expensive methods of fabrication.
- As these are internally placed, they pose challenge for using in long term cases [21]. Fabrication methods and the characteristics of the materials used also impact on its durability.
b. Electrocorticography (ECoG)
Intracranial electroencephalography is a technique for recording brain signals by putting electrode grids on the cortex’s surface. ECoG is an invasive BCI recording method that records with electrodes put directly on the brain’s exposed surface [22]. These are used when performing an internal brain surgery.
- They are expensive.
- They are bulky.
- They are prone to the formation of scar tissue, which obstructs the signal when the body reacts to the foreign item.
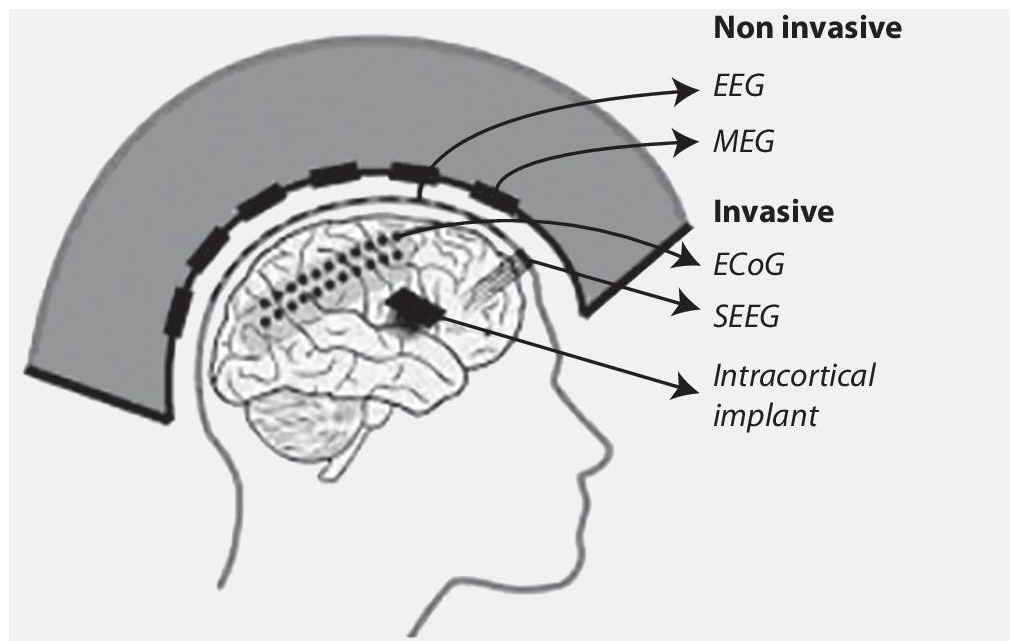
Figure 1.5 Recording places in/on brain.
- Limited sampling time – Seizures may not be recorded with EcoG [23, 24].
- The region of the exposed cortex and operation duration restrict the number of electrodes that may be placed. Errors in sampling are possible.
ECoG is a minimal invasive method. Stereotactic electroencephalography (sEEG) also used electrodes to measure brain activity. sEEG provides measurements from much deeper brain structures than ECoG, yet it has received very less attention in BCI applications [25, 26]. All, the intracortical, ECoG and sEEG are invasive methods and their placing in cortex is as shown in the Figure 1.5. ECoG is sometimes referred as semi-invasive method.
1.3.1.2 Non-Invasive Methods
a. EEG (Electroencephalogram)
EEG is a method of signal acquisition that records the electrical signals of the brain by the help of metal discs(electrodes) that are attached to the scalp [27]. There are four types of electrodes:
- Traditional wet electrodes
- Dry electordes
- Active electrodes
- Passive electrodes
Hardware concerns with EEG-based BCI equipment with wet electrodes:
- Maintenance and use of wet electrodes is cumbersome.
- Electrical impedance of the skin has its impact the signal acquisition, that is the quality of recording the brain signals. The water content in association with the electrodes reduces electrical impedance whereas the air in association with the electrodes increases the electrical impedance.
- The interface betweeen the skin and electrode causes noises which considerably affect the signal.
- The setup of wet electrode is not well tolerated by subjects over longer periods of recording a) because of the electrolytic gel used which causes irritation to the subjects b) because of the discomfort caused by the elastic straps to hold the eeg cap in place [28].
- The electrical impedance also depends on various factors like surface area of the electrode, room temperature, and the interface layer.The people who were taking the EEG readings must keep all these factors in check.
Hardware concerns with EEG-based BCI equipment with dry electrodes:
- The Quality of the signal obtained using dry electrodes is low when compared to wet electrodes [29].
- For dry electrodes the electrical impedance deteriorate rapidly with use and generally should be replaced after 30 days of usage.
- The electrode caps are prone to movement since there will be no gel to hold the caps in place.
- Highquality electrode caps are generally made of gold and titanium, for prolonged hours of usage change of electrode caps is recommended so it will be costly to buy and maintain the electrodes [30].
- Elastic straps are used to maintain the electric caps in place which causes discomfort to the subject over longer periods of time.
b. MEG (Magnetoencephalography)
It is an imaging test which reflects the activity of the brain by recording the magnetic fields produced by electric currents occuring naturally in the brain [31].
Hardware concerns with MEG-based BCI equipment:
- The MEG equipment is very expensive.
- MEG equipment requires liquid helium to maintain its superconducting equipment.
- The equipment must be used in a magnetic shielded room and the food used by the subjects and the examiner must also be administered ad managed.
- The patients need to remain relatively still during a MEG examination and the patients with a vagus nerve simulator, pacemaker, or similar device may not be able to undergo an MEG study [32].
c. Functional Magnetic Resonance Imaging (fMRI)
This method acquires the brain activity parameters based on blood flow changes. So, this method depends on cerebral blood flow coupled with neuronal activation. When brain is in use, the blood flow varies depending to the task being performed. Hence, the parameters also vary. fMRI is used to detect and evaluate the brain abnormalities that could not be captured in other imaging techniques like x-ray or MRI.
d. Near-Infrared Spectroscopy (NIRS)
This method measures brain activity in frontal cortex. Here light absorption is used to calculate oxygen and hemoglobin levels.
Before extracting the features from the measured parameters, pre-processing is required. Pre-processing generally consists of Referencing, temporal filtering, and signal enhancement. Referencing is comparing the measured brain signal to a standard or reference signal in the form of voltage. It can be common reference, average reference, or current source density. Temporal filtering removes unwanted noise signals that are present in the measured brain signals. Signal enhancement techniques like Principal component Analysis (PCA), Surface Laplacian, automatic enhancement methods are used to enhance the parameters measured.
1.3.2 Feature Extraction
Based on the signal processing, the commands are generated. So, identification of correct features is an essential step. Feature extraction in BCI is recognizing the events or useful properties that are captured by various neuroimage methods. This will reduce the complexity and help in classification. Generally used method is EEG and in feature extraction, frequency information of each electrode and between electrodes is extracted.
The noise and the outliers are important features of brain signals. Along with them, we also have to consider that brain signals are highly dimensional, timely information, non-stationary and non-linear. Particularly for EEG, the data collected is time series. There are EEG bands based on frequency range. These bands are Delta for frontal lobe, theta for temporal and parietal lobe, Alpha for occipital lobe, Beta for frontal central lobe, and Gamma for parietal lobe [33]. These bands are used in feature extraction.
A cross correlation is analyzed between different frequency bands and it helps to extracts few important properties. It is observed that Fourier transforms are not efficient when the signals are non-linear and nonstationary, so time-frequency methods are used in feature extraction, like wavelet algorithm (based on the physiological activity knowledge) and empirical mode decomposition.
Any EEG signal has features that are measured in time domain. These parameters are referred as Hjorth parameters that basically are activity, mobility, and complexity. In addition to this, parametric models are used to model time series. Autoregressive parameters, Multivariate autoregressive parameters, adaptive autoregressive parameters and these parameters with exogenous input are considered [34].
There is another set of models called Inverse models. These models represent the brain as a set of volume elements called as voxels. Specific patterns are identified in the regions associated with cognitive component. These are the peak picking methods. Another method is the slow cortical potentials calculation in which amplitudes are extracted, corrected, and used as feedback.
Poor feature detection and extraction would reduce the accuracy and efficiency of the BCI model. The feature extraction of brain signals directly depends on the signal types being measured and recorded. Along with the above mentioned feature extraction, commonly used features include mean, slope, peak, signal minimum, skewness, and kurtosis, number of occurrence of peaks, variance, root mean square, standard deviation, median, power spectrum density (PSD), logarithmic band power and common spatial patterns [13].
1.3.3 Classification
The signal patterns in the brain are dynamic stochastic processes because of the biological factors and technical issues like amplifier noise and electrode impedance changes. The identified signals before being translated into commands have to be classified. That is grouping of the signals based on their appropriate features. There are many categories of classification algorithms used in BCI systems. With the advancements in Artificial Intelligence, Machine Learning (ML) and Deep Learning (DL), more advanced algorithms for feature extraction and classification are in use.
There are four classifier taxonomies in contrast to each other.
- Generative/Informative and Discriminative classifiers
- Static and Dynamic classifiers
- Stable and Unstable classifiers
- Regularized classifier
1.3.3.1 Types of Classifiers
1. Linear Classifiers
These classifiers use linear algorithms to differentiate between two or more classes. A hyper plane is used to distinguish the considered data falls in first or second class. The classic examples of linear classifiers are Linear Discriminant Analysis (LDA) and Support Vector Machine (SVM).
Linear Discriminant Analysis is a popular classification algorithm used in BCI applications. It is a dimensionality reduction technique. LDA uses single hyperplane to separate the data representing the two classes and several hyperplanes if multiclass problems are used. The discrimination rules used in LDA are “maximum likelihood”, “Bayes Discriminant Rule”, and “Fisher’s linear discriminant rule”. This method is used because of its very low computational requirement and as well provides good results.
Support Vector Machine was originally designed for binary classification and to maximize the margin compared to LDA. SVM uses statistical learning theory. It searches the maximum margin hyperplane between two classes. Maximization of the margins extends the generalization capabilities of the algorithm. The accuracy is improved by adjusting the parameters. A variant in SVM is the Gaussian SVM that provides excellent accuracy in classification.
2. Neural Networks Classifiers
A neural network is an arrangement of processing units in layers that convert the input to output using weights associated with the nodes. These are commonly used classifiers for BCI along with linear classifiers. Multi-Layer Perceptron (MLP), Learning Vector Quantization, Adaptive Logic Networks, Time Delayed Neural Network, Recurrent Neural Network are few neural network classifiers. An MLP contains multiple layers of neurons in the form of an input layer, either one or more hidden layers, and an output layer. The neurons of the output layer determine which class the input feature vector belongs to (that is classifying which class). MLP classifies to any number of classes which makes neural network more flexible. It is also called as universal classifier and can be applied to most of the BCI problems that have either two (binary) or multiple classes to discriminate [35].
3. Non-Linear Bayesian Classifiers
Bayes quadratic, Bayesian Graphical network (BGN) and Hidden Markov Model (HMM) are the Bayesian classifiers used for BCI: Although Bayesian Graphical Network (When compared BGN is slow compared to other two. Hidden Markov Models are very efficient nonlinear techniques used for the time series data or signal classification. HMMs are the dynamic classifiers that are used for speech recognition. HMMs work on a probabilistic automaton for a given sequence of feature vectors.
4. k-Nearest Neighbor Classifiers
k-NN classification is a non-parametric model in which a new feature is assigned to a class depending on nearest neighbors. It is described as instance-based learning where the model memorizes the training datasets. It provides better accuracy in classification with less training and testing datasets. Features of EEG signals can be extracted by Hjorth’s parameters like activity, mobility and complexity are extracted and, on that k-NN classification would result in improved accuracy. First the number of nearest neighbors is found and then data points are classified based on that. Euclidean distance is used to find the neighbors. It selects k samples from training set. This classifier is based on giving new samples to the class with majority of votes [36, 37].
1.4 Applications of BCI
BCI has taken a big leap in its applications with the growth in modern computing and cognitive levels of humans in understanding the brain. BCI applications are making the unconquered world into reality. With BCI, it is possible to manipulate the thoughts with computers. BCI, in its nascent days involved recording brain signals, in contrast to designing implants in today’s world. These implants act as a communication tool between the brain and outside world. Implants are designed for some important brain functions such as feeling, hearing and vision to name a few.
Earlier BCI was used for decoding the thoughts of the handicapped people with speaking and mobility issues. These applications used methods such as speech communications and spelling applications that aided as an alternative means of communication. With modern computing, BCI is even used for healthy people. Now days, BCI is used as measuring tool to assess an individual’s physiological quotient involving emotions, cognitive level and effectiveness.
Just as the brain functions in diverse areas, BCI applications span over a diverse area such as Healthcare, Education, Smart environment, Security and authentication, Marketing and advertising, Gaming and entertainment. Since BCI acts as a medium between the brain and the outside world, its application domains are infinite and very promising i.e., BCI applications are to be considered that are pertinent to specific business.
a) Healthcare
Healthcare applications of BCI have transformed to various clinical products used in daily life. BCIs can be classified under the clinical uses as the direct assistive control technologies and neuro rehabilitation. These assistive control BCI applications encircle areas of communication, locomotion and movement control, environment control, prevention, detection and diagnosis [38].
b) Communication
BCI is mainly used for communicating with people with locked-in syndrome. Three types of BCI systems based on EEG, that measure electrophysiological features tested on humans for commination purpose are: Slow Cortical potentials (SCPs), P300 event-related potentials and senso-rimotor rhythms (SMRs) [38].
c) Movement Control and Locomotion
Paralyzed patients can restore their motor control with BCI. This scanty clinical application is solely based on SMRs. These applications support the controlled movement of motor neuro prosthesis in multidimensions such as robotic arm. Also, for paralyzed patients with intact lower motor neuron and peripheral nerve function, restoration of motor functions is done with Functional electrical stimulation (FES). BCI driven wheelchairs are used for restoring mobility for paralyzed patients. These wheelchairs control mental activities of the patient with a shared control system which use intelligent software for assisting the patient in navigating the wheelchair [38].
d) Prevention
BCI are used in various consciousness level detection system. These applications prevent loss of function and decrease in alertness level which are the side effects of smoking of due to consumption of alcohol. BCI is also used in detecting motion sickness, which arise due to confliction of sensory generated between eyes, ear and brain during motion of the individual [39].
e) Detection and Diagnosis
BCIs are used in monitoring mental state for detecting and forecasting of abnormal variations in the brain structure such as brain tumor, brain selling, seizure, and sleep disorders. BCI uses EEG in contrast to MRI and CT Scan for discovering tumors, which develop basically because of self-dividing of cells. Plantar pressure measuring systems exploit the relationship between the human gait cycle and EEG signals for diagnosing dyslexia, peripheral neuropathy and musculoskeletal diseases [39].
f) Rehabilitation
Patients with mobility issues are given physical rehabilitation for restoring the lost functions and regain their previous mobility levels, so that they can adapt to the disabilities. With these physical rehabilitations, patients suffering from strokes can also recover fully. BCI uses mobile robots for eases the daily life activities of such patients. BCI based neuro-prosthetic devices are used for patients wherein their previous levels of communication or mobility cannot be recovered. Nowadays BCI is diving into the arena of virtual reality for monitoring and controlling the avatar movements generated from the brain waves. Augmented reality-based BCI system such as augmented mirror box uses brain signals that are generated by incorporating both the injured as well as healthy limb. BCI driven therapeutic tools have the potential to the aide patients with impaired neuro muscular functions because of trauma, to re-learn the motor functions. These BCI systems enable patient’s functional recovery and thus enhance their quality of life [39].
g) Education
In BCI enabled education systems, brain signals are used to understand the level of clarity in processing the information. Non-invasive BCI techniques are used for self-regulating the learning experience and improve the cognitive therapeutic methods. fMRI-based EEG BCI trainings are used for emotional regulation, fight depressions and other neuropsychiatric disorders [39].
h) Smart Environment
Severely disabled patient’s quality of life can be improved significantly with BCI-based environment control system. These control systems effectively manage their daily life environment around them such as lighting systems in the house, room temperature, TV units and power beds. Smart environment systems enhance the patient’s well-being and relieve them from being dependent on others. Smart environments based on BCI enhance well-being, safety, and independence of patients in daily life. Modern computing has tied up BCI technologies and Internet of Things (IoT) that create smart houses, workplaces, and transportations for monitoring the patient’s mental state and adapt the surrounding environment appropriately. These functionalities are extended to use of universal plug and play home networking. Working conditions can be greatly improved by assessing the user’s cognitive state. BCI systems are used for studying the impact of mental fatigue and stress levels because of workload. Various BCI techniques are used in assessing the user’s cognitive state. Even virtual audio-visual set-ups are used for analyzing and evaluating the brain signals associated with the user’s response [39].
i) Security and Authentication
Authentication in security systems is based on algorithms, objects, and biometrics. Such systems are vulnerable to attacks because of the use of insecure passwords, surfing, spoofing and data theft. Cognitive biometrics is making space in the field of security and authentication, as they possess least vulnerabilities. Cognitive biometrics, also termed electrophysiology, is the only modality that uses brain signals for identifying the data in secured manner. Security is greatly enhanced in cognitive biometrics, as brain signals cannot be acquired by the hackers. Cognitive biometrics are difficult to synthesize and in turn enhance the biometric systems resistance to spoofing attacks [39].
j) Marketing and Advertising
BCI technologies have also conquered the marketing and advertising domain. BCI systems enable to measure a user’s attention when watching a TV commercial or any other channels. These measures try to assess the impact of user’s cognitive function in the neuromarketing and advertising field. BCI systems are also used to estimate the user’s inclination for TV commercials and use the same for advertising [39].
k) Gaming and Entertainment
Non-medical BCI has invaded the entertainment and gaming arena. The brain controlling capabilities combined with the gaming features provide experience of involving multiple brains. A game called Brain ball was developed for reducing stress levels in individuals. This game involves a user moving the ball only in relaxed mode. In this game, only a calm player can win the game, as they need to control stress and play [39].
1.5 Challenges Faced During Implementation of BCI
In the recent years substantial research is seen to develop BCI assistive technologies. In BCI invasive and non-invasive research is growing fast and a number of challenges are to be resolved to have lower impact on the patients. A number of neurosurgeons, neurologists, neuroscientists and engineers are investigating in this field for a significant breakthrough. There exist many challenges and issues in different areas such as technical, ethical, etc.
Even in recent times people are not deploying BCI in an effective way due to various obstacles faced such as ethical, legal, usability, and technical challenges. Challenges are also caused due to the signals received from brain activity are liable for intrusion, can also cause harm to patients controlling the device or an issue of protecting the data of the patient. In this section let’s discuss the challenges that affect the advancement in this technology.
A. Usability Challenges
It talks about the issue of acceptance by patients to use BCI technology. These usability challenges can be either issues related to training process or ITR (Information Transfer Rate) [1]. The user has to be trained to deal and control with the system and is a time-consuming process. This training is either in the preliminary phase or in the calibration phase. The most common available solution to this is to adopt single trial instead of multiple trials. One of the solutions is to use zero training classifier.
Information Transfer Rate is the method used widely for evaluating BCI systems. This parameter depends on the accuracy of detection, the number of trials and the average detection time taken. Increase of accuracy of detection can be achieved by increasing signal to noise ratio and should be considered in pre-processing phase. An approach called dynamic stopping is use to reduce average detection time is certain applications. Another method to reduce average detection time is to use single trail classifier which uses machine learning. Healthier individuals’ groups have higher data rates as compared to disabled.
B. Technical Challenges
These are related to recording of the electrophysiological properties of brain signals. The technical challenges include the issues related to non-linearity, noise, non-stationary, quality of the dataset, limited number of training sets, data fusion, inability of data interpretation
i. Non linearity: The function of the brain cannot be thought as a serial machine which reads the input from sensors and gives a corresponding output. Brain is a complex machine which can be termed as a memory-based predictive machine which by experience builds results depending on the relation between the inputs. Hence the signals from the brain are an ensemble of neural behavior which can be characterized as non-linear dynamic signals. Hence the machine representing a brain has to be dynamic and non-linear which remains as a challenge.
ii. Noise: It is another unwanted signal which causes random variation of the brain signals due to improper placement of electrodes, movement artifacts of skeletal muscles, blinking of eyes. This leads to improper analysis of the pattern. Removal of noise is carried out by using frequency band filters which will also remove the signal of interest lying in the same band.
iii. Nonstationary signals: The electrophysiological signals of the brain change continuously make it from minute to minute. During the recording session the emotional and mental state differ with different trials. Hence the EEG signals obtained can have varied signal levels over different sessions. Other nonstationary factors such as fatigue, concentration and stress produce varied EEG signals.
iv. Quality of the data set: In BCI application the quality of the EEG signals depends on the quality of the headsets or electrodes used for the measurements. The electrodes used for measurement usually requires gel or liquid which cause discomfort to users. Practically when user’s comfort is to be considered dry electrodes are preferred. Some investigations reports that the data acquired from dry electrodes consists of more noise when compared with wet electrodes whereas another set of studies reports that the quality of data are almost same for both electrodes. There is a need for further investigations on the usage and efficiency of electrodes for the validation of the data. Another investigation infers that the performance of water-based electrodes and dry electrodes are better than gel-based electrodes in case of short hairs. Hence the challenge is to determine the type of electrodes to be used by further investigations and validation [40].
There are numerous EEG head-sets available in the markets with different number of electrodes. The number of electrodes used for BCI applications varies with different companies and are not compatible with each other. Hence there is a need for standardization for number of electrodes. The cost of these electrodes is very high, hence requiring cheaper electrodes for BCI applications.
v. Limited number of training sets: The efficiency of the BCI system depends on the number of training sets used in a model. Small data sets can be used for training the model which has less complexity. Overfitting occurs when limited number of training set are used which in turn reduces the efficiency of the predicting models.
vi. Data analysis methods: There are numerous algorithms which are used for removal of artifacts in data pre-processing. Different algorithms have different limitations when used in analyzing the EEG data. Some algorithms focus on the removal of certain artifacts some focus on increasing the accuracy in the removal of artifacts. Different applications use different algorithms like ICA algorithms are used for artifacts removal in EEG recordings, CCA, and its combination for removal of muscle artifacts. When artifacts overlap with the spectral components then Wavelet transform fails completely. Hence the challenge arises for a single algorithm which can be efficient and accurate to satisfy different conditions satisfactorily. Thus, the goal for future researchers would be to develop algorithms which are application specific and has good accuracy and time efficiency and standardize the methods for a particular application [40].
In context to feature extraction techniques CSP and its combination algorithm gives encouraging results for EEG data. Based on the investigations done by researchers SVM is considered as the most powerful classifier powerful classifier for classification of high dimensionality feature vectors. Another study shows that the deep learning methods, CNN and RNN are better when compared with other methods and the accuracy of CNN is high for time-series values.
vii. Inability to interpret data: Another major challenge is to interpret data that is extracted from brain activity. There are numerous methods to extract information from the brain either through invasive or non-invasive methods. Usually in most of the cases the obtained data is partial or noisy. This may be due to unstable recording or due to built-in flexible nature of brain. Hence learning of neural signal processing is essential to understand the adaptive nature of the brain [41].
All BCI experiments are conducted in a controlled environment (lab) where realistic target users are not considered. Studies show that heart rate and cortisol influences characteristics of EEG data. EEG data varies with sensory stimulus such as smell, sound, and movements which affect the quality of EEG data. Hence in order to make BCI the system robust the engineers should consider the environment where the BCI system is applied along with the target set of users. For example, the design criteria change for a user who stays at home most of the times and controls household articles and for a person who is taxi driver who drives in a heavy traffic, the level of attention and concentration are different. Hence during design phase, it is important to consider the environmental aspects and the target user for a more efficient BCI system.
C. Psychophysiological and Neurological Challenges
The BCI performance depends on Psychological and neurological to a greater extent. The neurological factors such as anatomy and functional behavior vary from individual to individual. Similarly, the psychological factors such as memory, attention span, fatigue and stress also vary from individual to individual. Apart from these other characteristics such as gender, lifestyle, age also influences the brain signals. Hence a generalized approach to develop BCI without considering these aspects will decreases the efficiency [42].
D. Ethical and Socioeconomic Challenges
The factors such as safety, data confidentiality, and social and economic factors are to be considered to maximize the benefits to the users. The BCI user’s physical and mental safety should be considered as the most important aspect. One of the invasive procedures such as deep brain stimulation should not cause physiological and neurological effects. Bleeding and infections are caused when electrodes are implanted which in turn leads to behavioral changes. These invasive methods are sometimes potential threats to memory and emotions.
The target application of most of the BCIs is the disabled people. Hence the user’s expectation of attaining their freedom sometime may not be satisfied. Even a small risk can rule out the usage BCI system. Creating awareness in the users with advantages and disadvantages is an important social responsibility. During the implementation of BCI there can be alteration in human cognitive level is a serious ethical issue. During commercialization of BCI ethical and legal policy has to be maintained between the user and the service provider.
BCI has a lot of potential and growth opportunities. Its global market size is huge and it is projected to be close to $4 billion by 2027. Many start-ups and SMEs can pitch in this market with their innovative devices. The advanced technological developments have paved a way for BCI extensively in healthcare sector and other fields like entertainment, gaming and communication. As with any technology, there are certain issues with this BCI technology also, particularly ethical issues and we need to wait and watch how this technology would be utilized for the betterment of human-kind.
References
- 1. Vaidya, R.R., Nagendra, A., Shreyas, B., Munavalli, J.R., Predictive and comparative analysis for diabetes using machine learning algorithms. Int. J. Adv. Sci. Technol., 29, 3, 14407–14416, 2020.
- 2. Nalluri, S.P., Reshma, L., Munavalli, J.R., Evaluation of virtual reality opportunities during pandemic. 2021 6th International Conference for Convergence in Technology (I2CT), 2021.
- 3. Munavalli, J.R., Rao, S.V., Srinivasan, A., Manjunath, U., van Merode, G.G., A robust predictive resource planning under demand uncertainty to improve waiting times in outpatient clinics. J. Health Manage., 19, 4, 563–583, 2017.
- 4. Munavalli, J.R., Rao, S.V., Srinivasan, A., van Merode, G.G., An intelligent real-time scheduler for out-patient clinics: A multi-agent system model. Health Inform. J., 26, 4, 2383–2406, 2020.
- 5. Munavalli, J.R., Rao, S.V., Srinivasan, A., van Merode, G.G., Integral patient scheduling in outpatient clinics under demand uncertainty to minimize patient waiting times. J. Health Inform., 26, 1, 435–448, 2020.
- 6. Munavalli, J.R., Rao, S.V., Srinivasan, A., van Merode, G.G., Workflow-based adaptive layout design to improve the patient flow in the outpatient clinics. Ann. Romanian Soc. Cell Biol., 25, 3, 8249–8257, 2021.
- 7. Munavalli, J.R., Rao, S.V., Srinivasan, A., van Merode, F., Dynamic layout design optimization to improve patient flow in outpatient clinics using genetic algorithms. Algorithms, 15, 3, 85, 2022.
- 8. Shih, J.J., Krusienski, D.J., Wolpaw, J.R., Brain–computer interfaces in medicine. Mayo Clinic Proceedings, vol. 87, pp. 268–279, 2012.
- 9. Kummar, R.G., Suhas., S.J., Vismith, U.P.J., Munavalli, J.R., Brain computing interface-applications and challenges. IOSR J. Comput. Eng., 23, 2, 29–40, 2021.
- 10. Abdulrahman, S., Roushdy, M., Salem, A.B.M., Overview of acquisition techniques brain signals in human identification and disease diagnosis: Applications and challenges. TEST Engineering & Management, 83, 10564– 10575, 2020.
- 11. Batista-Garcia-Ramo, K. and Fernández-Verdecia, C., II, What we know about the brain structure-function relationship. Behav. Sci. (Basel, Switzerland), 8, 4, 39, 2018.
- 12. Cho, J., Jeong, J., Kim, D., Lee, S., A novel approach to classify natural grasp actions by estimating muscle activity patterns from EEG signals. 2020 8th International Winter Conference on Brain–Computer Interface (BCI), 2020.
- 13. Hong, K.S., Khan, M.J., Hong, M.J., Feature extraction and classification methods for hybrid fNIRS-EEG brain–computer interfaces. Front. Hum. Neurosci., 12, 246, 1–25, 2018.
- 14. Khanna, K., Verma, A., Richard, B., The locked-in syndrome: Can it be unlocked? J. Clin. Gerontol. Geriatr., 2, 4, 96–99, 2011.
- 15. Baek, C., Jang, J., Park, S., Song, Y., Seo, K., Seo, J., 3D printed wire electrode carrier for a pilot study of the functional brain mapping. 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), 2017.
- 16. Chuan, Z., Jingquan, L., Hongchang, T., Xiaoyang, K., Yuefeng, R., Bin, Y., Hongying, Z., Chunsheng, Y., Control of swimming in crucian carp: Stimulation of the brain using an implantable wire electrode. 8th Annual IEEE International Conference on Nano/Micro Engineered and Molecular Systems, 2013.
- 17. Gardner, A.T., Strathman, H.J., Warren, D.J., Walker, R.M., Impedance and noise characterizations of Utah and microwire electrode arrays. IEEE J. Electromagnet. RF Microwaves Med. Biol., 2, 4, 234–241, 2018.
- 18. Sharma, M., Gardner, A.T., Silver, J., Walker, R.M., Noise and impedance of the SIROF utah electrode array. 2016 IEEE Sensors, 1–3, 2016.
- 19. Kim, M., Park, S., Chung, W.K., Flexible polymer-based micro needle array sEMG sensor. 10th International Conference on Ubiquitous Robots and Ambient Intelligence (URAI), 2013.
- 20. Al-Othman, A., Alatoom, A., Farooq, A., Al-Sayah, M., Al-Nashash, H., Novel flexible implantable electrodes based on conductive polymers and Titanium dioxide. IEEE 4th Middle East Conference on Biomedical Engineering (MECBME), 2018.
- 21. Szostak, K.M., Grand, L., Constandinou, T.G., Neural interfaces for intracortical recording: Requirements, fabrication methods, and characteristics. Front. Neurosci., 11, 665, 1–27, 2017.
- 22. Krishnan, J., Rethnagireeshwar, R., Benjamin, B., Panicker, N.V., Ramu, A.R.B., High precision resistance spot welding with subdural electrodes for acute electrocorticography applications. IEEE International Conference on Power, Control, Signals and Instrumentation Engineering (ICPCSI), 2017.
- 23. Hill, N.J., Gupta, D., Brunner, P., Gunduz, A., Adamo, M.A., Ritaccio, A., Schalk, G., Recording human electrocorticographic (ECoG) signals for neuroscientific research and real-time functional cortical mapping. J. Vis. Exp., 64, 3993, 2012.
- 24. Yang, T., Hakimian, S., Schwartz, T.H., Intraoperative Electrocorticography (ECoG): Indications, techniques, and utility in epilepsy surgery. Epileptic Disord., 16, 3, 271–9, 2014.
- 25. Herff, C., Krusienski, D.J., Kubben, P., The potential of stereotactic-EEG for brain–computer interfaces: Current progress and future directions. Front. Neurosci., 14, 123, 1–8, 2020.
- 26. Young, J.J., Friedman, J.S., Panov, F., Camara, D., Yoo, J.Y., Fields, M.C., Marcuse, L.V., Jette, N., Ghatan, S., Quantitative signal characteristics of electrocorticography and stereoelectroencephalography: The effect of contact depth. J. Clin. Neurophysiol., 36, 3, 195–203, 2019.
- 27. Min, B., Eeg/sonication-based brain-brain interfacing. 2013 International Winter Workshop on Brain–Computer Interface (BCI), 2013.
- 28. Lee, S., Shin, Y., Woo, S., Kim, K., Lee, H., Dry electrode design and performance evaluation for EEG based BCI systems. 2013 International Winter Workshop on Brain–Computer Interface (BCI), 2013.
- 29. Yang, S.Y. and Lin, Y.P., Validating a LEGO-Like EEG headset for a simultaneous recording of wet- and dry-electrode systems during treadmill walking. 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), 2020.
- 30. Kim, D., Yeon, C., Chung, E., Kim, K., A non-invasive flexible multi-channel electrode for in vivo mouse EEG recording. IEEE Sensors, 17, 326, 1–14, 2014.
- 31. Waldert, S., Braun, C., Preissl, H., Birbaumer, N., Aertsen, A., Mehring, C., Decoding performance for hand movements: EEG vs. MEG. 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, 2007.
- 32. Lefevre, J. and Baillet, S., Mapping and tracking the flow of brain activations using MEG/EEG: Hypothesis and methods. 2007 Joint Meeting of the 6th International Symposium on Noninvasive Functional Source Imaging of the Brain and Heart and the International Conference on Functional Biomedical Imaging, 2007.
- 33. Manjula, K. and Anandaraju, M.B., A comparative study on feature extraction and classification of mind waves for brain computer interface (BCI). Int. J. Eng. Technol., 7, 19, 132–136, 2018.
- 34. Resalat, S.N. and Saba, V., A study of various feature extraction methods on a motor imagery based brain computer interface system. Basic Clin. Neurosci., 7, 1, 13–19, 2016.
- 35. Sridhar, G.V. and Mallikarjuna Rao, P., A neural network approach for EEG classification in BCI. Int. J. Comput. Sci. Telecommun., 3, 10, 44–48, 2012.
- 36. Anupama, H.S., Cauvery, N.K., Lingaraju, G.M., k-NN based object recognition system using brain computer interface. Int. J. Comput. Appl., 120, 2, 35–38, June 2015.
- 37. Bablania, A., Edla, D.R., Dodia, S., Classification of EEG data using k-nearest neighbor approach for concealed information test. 8th International Conference on Advances in Computing and Communication (ICACC-2018), 2018.
- 38. Mak, J.N. and Wolpaw, J.R., Clinical Applications of brain–computer interfaces: Current state and future prospects. IEEE Rev. Biomed. Eng., 2, 187–199, 2009.
- 39. Abdulkader, S.N., Atia, A., Mostafa, M.-S.M., Brain computer interfacing: Applications and challenges. Egypt. Inform. J., 16, 213–230, 2015.
- 40. Rashid, M., Sulaiman, N., Abdul Majeed, A.P.P., Musa, R.M., Ab. Nasir, A.F., Bari, B.S., Khatun, S., Current status, challenges, and possible solutions of EEG-based brain–computer interface: A comprehensive review. Front. Neurorobot., 14, 1–35, 2020.
- 41. Vaadia, E. and Birbaumer, N., Grand challenges of brain computer interfaces in the years to come. Front. Neurosci., 3, 2, 151–154, 2009.
- 42. Saha, S., Mamun, K.A., Ahmed, K., Mostafa, R., Naik, G.R., Darvishi, S., Khandoker, A.H., Baumert, M., Progress in brain computer interface: Challenges and opportunities. Front. Syst. Neurosci., 15, 578875–578875, 2021.
Note
- *Corresponding author: [email protected]