
Diana Santos Fernandes, Carolina Feliciana Machado
5Human resource management in the health system: in the never-ending quest for productivity improvement
Abstract: The need to pay attention to health human resources was underlined by the World Health Organization in its most recent assessment (2009) of the current national health program and performance of the Portuguese National Health Service (NHS) system. This chapter focuses on health human resource management (HHRM) capabilities in the Portuguese NHS to determine whether there is a paradigm of strategic management, concluding that it does not. We argue that there is a “myopia” problem in the standard of HHRM because it focuses on administrative costs and not on the broader workforce, which is able to give it sustainable competitive advantages. This study mostly uses the collection and analysis of secondary quantitative data, presenting the observed performance in human resource management in the Portuguese NHS compared to the expected (strategic HHRM), interpreting the results in a deductive way. We highlight the originality and value of this work as an analytical document and as a script to apply in the transition to a strategic HHRM approach in the Portuguese NHS.
Introduction
This chapter discusses health human resource management (HHRM) models, presenting as the research problem the analysis of the dynamics in the Portuguese National Health Service (NHS), in order to understand the reason for its inefficient performance. We aim to determine the possibility of the existence of a strategic management paradigm in this public sector; the reason we argue that the improper investment of the Portuguese NHS in its human capital, which can supply a sustainable competitive advantage, is the source of its inefficient performance; this will be the main working hypothesis.
Taking into account these issues, this chapter assumes a great relevance, as in recent evaluations the World Health Organization (WHO) had outlined weaknesses in Portuguese NHS management, focusing in particular on the challenges at the HHRM level, which can threaten its sustainability [1]. We also highlight recent dissatisfaction of users and workers with Portuguese NHS management. Indeed, for workers at a public service focused on human welfare, such aims are undermined by the excessively economic vision of its functions, which is guided by cost savings.
This research is divided into three sections. First we will develop a theoretical revision in the strategic human resource management (SHRM) field, focusing on factors that have encouraged the evolution of human resource management (HRM) policies and practices in the direction of this paradigm and its main characteristics, which will be crucial as a framework for this chapter. Having established this support, at the end of the first section we will present the adopted theoretical model as well as the corresponding hypothesis to guide our approach to the topic. The second section will explain the used methodology, focusing on the methods and processes of data collection and analysis. The third section will present the collected data and their analysis, discussing results in a deductive fashion. We will elaborate on a characterization of the HHRM model in the Portuguese NHS, comparing the corresponding observed and expected performances.
As we will see, the Portuguese NHS does not represent a strategic HHRM standard, and we will seek, in describing its actual standard, to show its gaps with a view to adopting the desired standard to achieve a more efficient HHRM. It is in this connection that we talk about the originality and value of this research: it is an analytical document and a guide with suggestions to be applied in the transition to a SHRM in the Portuguese NHS.
5.1Literature Review
5.1.1Strategic dimension of HRM
HRM consists in the close interdependence between a knowledge pool and an activity to achieve results, influencing the collaborators’ behaviors and attitudes through a management system. This comes from the growing awareness under which the organization of human capital can hardly be imitated, contrary to its traditional competitiveness factors, changing the role of workers, who become the strategic basis of the organization. In this way, we justify the relevance of SHRM on the premise, supported by empirical evidence, that organizational performance is influenced by the pool of HRM practices, defined and executed by the organization, with this assumption serving as the basis of the theory as well as of the research to be presented [2].
In the last decade HRM has become increasingly recognized as an important part of business, as its conceptualization developed from the concepts of costs, administration, training and collective negotiation to another based on the concepts of investment, management, development and teamwork. Such a change in paradigm reveals, indirectly, the erosion of traditional competitive factors, showing, directly, the importance of considering human resources (HR) as a competitive and strategic advantage in an organization’s survival. HR can act, in the view of Wright and MacMahan [3, p. 93], as “human capital.”13The authors propose that it will serve as a mediator between performance and HRM practices once the relation between these last two named issues is established as empirically demonstrated in the literature, for instance, in the work of Combs, Liu, Hall and Ketchen [4]. Lengnick-Hall and Lengnick-Hall [5], in accordance with the aforementioned authors, clarify the concept of competitive advantage, arguing that it is related to capabilities, resources, relations and decisions that allow an organization to capitalize on opportunities and avoid competitive threats within the sector in which it operates, which will require the adoption of SHRM.
The contemporary HRM vision arose after the 1990s, as organizations faced a multitude of technological, economic, social and political-legal challenges and needed to reorganize themselves at the structural and management levels to survive in the markets. The HR function developed and sought answers to current challenges through the reconciliation of economic options, the desire for profits and HR evolution, which is why, in this context, organizations focus on internal resources, assuming from that point forward that HR would be their first strategic resource. Organizations placed a bet on SHRM, according to Lengnick-Hall, Beck and Lengnick-Hall [6], that organizations would become more resilient, more competitive in the current international environment, and increasingly complex as a result of globalization.
Developing a critical literature review we verify that this idea is systematized by Wright, Dunford and Snell [7], solidifying organizational theory. We then emphasize how organizations understand their internal resources, which create value for them, leading to sustainable competitive advantages, as systemic imitation requires an understanding of exactly how all its elements interact, which is difficult, rendering infeasible the simple copying of isolated policies of competitors.
Related to this perspective, Ulrich [8] presents another theoretical categorization, proposing an organizational orientation toward key competencies, following the development of decentralized processes of decision making, since this stimulates workers’ greater commitment and motivation. These ideas are systematized by Pfeffer [9], who proposes that HR needs to play a new role in organizations, taking a central part, not in traditional activities, such as hiring, remuneration, or administrative support, but by developing enriching and useful solutions to organizational issues since HRis an “invisible asset” that can bring sustainable competitive advantages. To this end, Huselid and Becker [10, p. 426] suggest that SHRM adoption must be articulated in the following steps: operationalize strategy, operationalize strategic capabilities, operationalize strategic jobs, measure workforce differentiation, implement an HR architecture, determine impact of workforce differentiation on employees, integrate qualitative and quantitative data collection and analyses – all this in order to stimulate organizational performance improvement.
We live in a time of large-scale economic, technological and social changes, where information access, volume and speed are increasingly difficult to absorb both by individuals and organizations. Thus, the urgency of systemic thinking to understand this more complex environment due to globalization seems all the more pressing. On one hand, systemic thinking is understood as an interesting field of reasearch, on the other, it is also possible to observe challenges that can constraint knowledge evolution in this subject.
Systemic theory, applied to organizational activities, has had a huge impact on SHRM progress. Given the interdependence among HRM policies and practices, it is necessary to focus on its conceptualization as a coordinated system in order to analyze its impact on organizational performance, which requires that the system be greater than the simple sum of its parts: it is only by the interaction of the parts that specific characteristics will emerge, which is why Jamrog and Overholt [11] emphasize that the key to a theoretical approach to HRM lies in the mutual interaction of the different parts of the system.
Thus, research interest in HRM policies and practices systems and their impact on organizational performance has been increasing, on the assumption that the key to organizational success lies in the mutual satisfaction of collaborators and organizations’ interests and needs. We are witnessing a new conception of HRM in organizations, assuming a work force highly involved in organizations, highly flexible in their roles and skills, focusing on such key issues as selection, socialization, training and reward systems development [12].
According to Wright and McMahan [13], SHRM is being undermined by severe critics since without a strong theoretical basis to understand specific SHRM policies and practices, it is difficult to distinguish SHRM from traditional HRM. Nonetheless, the efforts aimed at SHRM theorization are motivated by a recognition of the strategic and symbolic dimensions of the human factor and its impact on organizational efficiency, since human capital is conceived as an invisible asset in organizations. This follows Pfeffer’s [9] ideas on the dynamic and relevance of organizations’ sustainable competitive advantages.
Despite the failure of academic researchers thus far to agree on a definition of SHRM, there is a broad consensus that such policy aims to achieve a match between HR and organizational skills, developing them mutually, taking into account that one will incentivize the other, in a logic of interdependence.
In Watson’s (1985, as cited in [14]) perspective, both concepts (HRM and SHRM) distinguish themselves in the value system that they advocate: due to the work force hierarchical control, promote workers’ commitment and autonomy in organizational activities, explain why paradigm metamorphosis requires the establishment of a different psychological contract based on reciprocal interactions as well as on high levels of trust and mutual satisfaction. The difference between paradigms is visible in the adoption of opposite HRM policies and practices. Work force planning is undergoing a transition from that of a “police nature” developed by supervisors to one that is participative, proactive, strategic, integrated and having a long-term dynamic. The self-regulation paradigm contrasts with this by its opposition to external control, as well as individual relationships on a basis of trust and not of intimidation or retaliation. It privileges flexibility and versatility of roles and sees HR as something to invest in, as opposed to a monolithic HRM concerned exclusively with cost cutting.
In accordance with the growing awareness that the social and economic domains are very closely interconnected – a consequence of globalization dynamics – SHRM is legitimized as a concept, as supported by Prahalad and Hamel’s [15] reflection that in this model jobs and skills are better integrated, with HR having a dynamic vision of organizational resources. The concept of competence becomes essential for achieving organizational success, as success must happen increasingly in an environment that remains turbulent and is undergoing continuous change: the contemporary globalized environment. Therefore, in the new HRM policies and practices, increasingly of a strategic nature, organizations focus on customization, adaptation, mobilization, sharing and anticipation, issues that will be discussed in greater depth when we present the theoretical model that supports this chapter [16, p. 34].
Ulrich (1996, as cited in [14, p. 52]) systematizes the two main vectors whereby HRM policies hang together: the strategic (long term) and the operational (short term), where SHRM activities should embrace individuals, in such processes, as a whole. To articulate even more the degree of systematization of this theme, Tavares and Caetano [14, p. 52] present, referring to Ulrich (1996), the four main aims of SHRM, combining the aforementioned strategic and operational axes: SHRM, transformational and changing management, organizational infrastructure management and worker contribution management. Thus, SHRM is both a concept and a set of practices, which is why it is so complex.
5.1.2Theoretical framework definition and research hypothesis
In our understanding, health human resources (HHR) has a twofold dimension, where capital plays a dual role of individual and agent of health care practices. A health system is grounded in three different types of capital – structural (health organizations), professional (HHR) and citizens (users) – and it is from their interaction that knowledge is created, based on the structural capital system and shared information and on citizens and the organizational professionals’ existing knowledge. This results in an increase in organizational intellectual capital, which requires coordinated action by all actors in management policies and practices [17].
To achieve the goals proposed in this chapter, we have elaborated a theoretical model considering the inputs given by three different authors, which is represented in Figure 5.1.
This was the option that resulted from some gaps found in an initial theoretical revision that we made on this topic. Indeed, it was not possible to find in the literature HRM models of analysis specific to the health care sector, as this thematic is, in this knowledge field, very recent. It was only possible to find general standards that must govern SHRM, not as applied to a specific field of activity, as well as specific characteristics that management in the health care sector obey, applied, however, to some particular national contexts. Moreover, and according to the preceding literature review, we also observed that the debate about SHRM remains, which is why, to overcome these constraints, it was necessary to develop a specific theoretical model adapted to the main aims of this study.
In what follows, we present the adopted theoretical model and its dynamic in what concerns the analysis of the problematic examined in this chapter. We adapt Dussault and Souza’s [17] theoretical model on the logic of the analysis of the situation with HHR because it provides analytical categories for understanding HR dynamics in a health unit, in which health goals are attained in a particular moment and in a specific context. To this end, the authors highlight three main processes at the HHRM level.
Competencies development refers to the knowledge production process and the competencies necessary to “achieve the levels of performance required by the health services goals” [17, pp. 13–14] in each professional category. Worker distribution focuses on the professional allocation process in different services, regions and subregions of the country, ensuring equality of access to all services for the entire population. About personnel management it looks to “guarantee an appropriate work environment and an adequate level of performance” of HHR [17, p. 23].
At the base of health sector HRM policies and practices (applying the development of a theoretical model to the specific context of analysis in this work, the Portuguese NHS) lie many relevant inputs that constrain them, namely, external (e.g., health episodes at the international level that have repercussions in the national reality; governmental policies that affect NHS regulation – financial, recruitment, rewards) and internal (e.g., ministry of health policies, already established power relations in the NHS and HHR). These inputs will have repercussions in HRM policies and practices in the NHS at the distribution, management and competency development level of the respective HHR. Thus, “all decisions, actions and inactions that affect production, distribution and personnel management are policies that need to be taken into consideration given the HHR analysis of situation” [17, p. 14]. Although this issue is considered in Dussault and Souza’s model, we have decided to develop and clarify it, adapting it to our specific case study.

Fig. 5.1: Scheme of adopted theoretical model. The logic of the situational analysis of HR in the health sector, particularly in the Portuguese National Health System (NHS), taking into account its management according to a strategic paradigm. (Source: Adapted from [16, p. 54]; [17, p. 13])
The coordination of all participants is required in the planning and execution of policies and practices in the health sector, as each decision dimension is, according to its nature, the responsibility of individual actors. Then the two previously mentioned inputs are correlated since the resulting external dynamics and orientations will be configured around the internal environment, providing more or less favorable conditions for the further implementation of HHRM. This is one of the changes (or better, clarifications) that we have inserted in the theoretical model of the cited authors.
Noting that such a model will be incomplete in terms of the present research, considering the hypothesis that we put forth (see end of this section), we have decided to introduce into the basic theoretical model the contributions of Peretti [16, p. 34], which will provide the key vectors by which an organization can maximize its performance, focusing on SHRM. By adaptation the organization will address internal and external requests through the use of different types of flexibility. Mobilization applies to the involvement of all hierarchies in HR commitment, which goes through information generation and dissemination, opening up options and means of solving problems. In turn, customization embraces global rewards, training and information; career, competencies and time management, reconciling workers’ expectations with organizational constraints. Sharing ensures that all managers take part in HRM in collaboration with the director of the corresponding job that will promote the new concept of a shared job. By anticipation we reinforce the need for forward-looking job management in the medium and long terms, taking into consideration environmental unpredictability.
Explaining generally the dynamic of the adopted theoretical model, we verify that Peretti vectors that lead to SHRM in the Portuguese NHS must be applied in each of the processes of Dussault and Souza in the situational analysis of HHR in this service. Such processes will require a set of inputs, influencers of the dynamics that we can verify in each of them. Only by this logic will we attain efficient organizational performance in the Portuguese NHS, therefore we will be able to detect if in the Portuguese NHS is presently applied a SHRM model, appearing from this conclusion the reasons that underlie to its inefficient performance.
Taking this into account, we have established a research hypothesis whose theoretical fundamentals lie particularly in Huselid, Jackson and Schuler’s [2] reflections. Based on the heterogeneity premise among organizations on what concerns human capital, competitive advantage is possible only if an organization guarantees that the added value that is possible as a result of activities performed by its workforce is seen as a unique resource, difficult to imitate and replace, as we emphasized in the theoretical review section. In this vein, SHRM practices embrace activities through which the organization generates human capital able to achieve these conditions and in this way promote positively organizational performance. Then, SHRM activities will serve as the means to achieve efficiency because they will help to ensure that the organization’s HR will not be easily imitated due to the complexities of culture and social dynamics and causal ambiguity inherent in SHRM practices, such as empowerment, schemes based on team collaboration, and long-term talent development, among other factors.
Thus, such arguments suggest the following mutually exclusive hypotheses:
H0: The Portuguese NHS presents a standard of SHRM that demonstrates that its performance, in terms of its HHR labor, will be efficient.
H1: The Portuguese NHS does not present a standard of SHRM that demonstrates that its performance, in terms of its HHR labor, will be inefficient.
The observed performance in the Portuguese NHS, in terms of the labor performance of its HHR, is the dependent variable, and the existence and application of an SHRM model will be the independent variable.
5.2Methodological considerations
This study articulates descriptive research, aiming to determine the HRM standard in the Portuguese NHS, presenting phenomena as they are in reality. In this case, it is necessary to collect a data set so that, based on a theoretical model that provides tools related to the dynamic of an SHRM model, it becomes possible to identify variables and inventory facts that make it possible to conclude whether or not the HHRM standard in the Portuguese NHS is strategic. Thus, this research follows deductive logic as it develops from a conceptual and theoretical structure that is later tested based on empirical observations.
The adopted research process emphasizes a quantitative feature since it is mainly concerned with collecting statistical data and assembling and analyzing numerical data, although other data of a qualitative nature may also be relevant to our study. The research adopts a positivistic paradigm, starting from the assumption that research develops in a logical direction, deducing that an act of researching reality has no effect on that reality, as the researcher seeks facts and the corresponding causes of social phenomena, placing little importance on the subjective position of the person.
In terms of the results, this study’s focus is basic research, as it looks to contribute, generally, to the scholarly knowledge base in the field of HRM modeling, with a special emphasis on strategic models, in the health field. However, this study also could serve to stimulate, in future research, the development of objective measures that would act as a guide in the implementation of SHRM in the Portuguese NHS or in other similar contexts. In this vein, this study could, in future research, see further development with a more applied character. We highlight its originality and value as it is assumed not only as an analytical document but also as a guide to be applied to behavioral changes, bearing in mind SHRM in the Portuguese NHS.
The data to be collected are largely quantitative and secondary in nature and focus on the statistics presented by the Portuguese Statistical Institute (INE). Other sources include research reports and surveys that make observations on issues specific to HHR as elaborated by the Portuguese Medical Association or the Portuguese Nurses Association.We have also used official information released by the Ministry of Health, projections elaborated by the Portuguese Central Authority of Health Services (ACSS), as well as Portuguese legal documents. Contributions from scientific books and journals and other studies addressing this theme were also used. This was necessitated by the dearth of information on the subject available for study and by the difficulties in accessing the information, as well as the need to collect the maximum amount of information about the past and current situation of the Portuguese NHS. This will be a limitation of the present study, which is why the methods used in data collection were based on the analysis of documents and bibliographical filtering, since primary data could not be gathered and other data collection mechanisms that would have allowed us to conduct a more in-depth analysis of the data at our disposal were not available.
Data was collected in the 2000s and 2010s because it is important to use data from a reasonably long but also relatively recent period of time. In this way, the subsequent data analysis will allow us to extrapolate, in a more reliable way, evolving trends in the Portuguese NHS, in terms of its HRM. Thus, this research represents a longitudinal study.
With such data, we intended to collect information about the performance of HHR in the Portuguese NHS, in each of the processes of the adopted theoretical model, in an attempt to determine its present HRM model (which we call “observed performance”).
Indeed, to analyze the process of HHR competency development, we undertook the collection of evidence relative to Portuguese HHR training, in part relative to all newly trained HHR, to the content and length of training, to the constraints on doctors and nurses regarding the formal launching of their careers, and to the accreditation agencies of the education establishment. To analyze the process of HHR distribution, we gathered evidence on the surplus or shortage of health professionals, as well as of HHR personnel based on nationality and region of the country where they work. Also important was the amount of HHR allocated to provide primary and secondary health care and relative to the share of HHR based on clinical or professional category, and further the amount relative to provider-to-patient ratio by type of service. To analyze the HHR management process, we analyzed the criteria used in worker allocation, working hours, legal documents in Portuguese NHS management, HHR recruitment methods in public services, and the (non-)existence of incentives for improving distribution and staff retention.
The analysis and further interpretation of data were processed using deductive logic (supported by the assumptions of the adopted theoretical model and the information mentioned in the earlier literature review), through content analysis, looking to elaborate on an actual performance description of the Portuguese NHS, occasionally also using a comparative methodology. This strikes us as an appropriate approach since we base our analysis on a longitudinal study in terms of a time period comparison to extrapolate the behavior standards of the involved variables, defining them, describing their behavior, and outlining their evolutionary dynamic.
Yet, based on the analysis and corresponding descriptions of HHR performance in the Portuguese NHS, we will reveal the observed performance (present) in its management. Articulating the presented data analysis methodology, we will verify whether that performance matches the expected performance, which will focus on SHRM. In the present study it will not be possible to analyze each of the aims in the health sector. Thus, our approach consists in emphasizing the comparison of the observed and expected performances with respect to HRM in the Portuguese NHS. In addition, we argue that efficiency will be possible only in a certain context and at a given time if SHRM is adopted.
5.3Data presentation and analysis and discussion of results
5.3.1Processes in the logic of HHR situation analysis in Portuguese NHS
In what concerns HHR competency development, we have verified that continuous professional development covers all health professions, answering to the educational needs of different elements of a multidisciplinary work team within the quality improvement scope of the health unit concerned (Pringle, 2000, as cited in [18]). However, the transition to this paradigm never happened in the Portuguese NHS [19].
Most educational institutions that develop training in the health care field are accredited. However, a significant number of such institutions are only in the preliminary stages of accreditation. There are extensive training requirements and a series of professional self-regulation procedures by multiple entities that require evaluations between different professional degrees that do not belong in programs structured and articulated by local training departments, much less entail improvements in the health units’ quality. The approval to open up courses in the health field, in the public or private sector, as well as the establishment of a limited number to accede to the university, or in available jobs to medical or nursing specializations in the country, is limited by governmental directives, which limit the existence of a higher workforce in the Portuguese NHS (Rodrigues, 2002, as cited in [18, p. 286]).
Between 2000 and 2010, admissions to training programs for doctors, nurses, dentists, and pharmacists saw continual growth. The number of trained specialist doctors has clearly grown, at a rate exceeding 120% between 2005 and 2010. The annual average growth of university graduates between 2000 and 2008 is positive in these professional categories, except for pharmacists in 2004, which saw a decrease of 41% [20, p. 23–25].
With regard to HHRdistribution, since 2002 we have witnessed continual growth in the number of doctors, nurses, pharmacists, and dentists. The ratio of nurses to doctors from 2002 to 2010 remained constant at 1.2 [20, p. 23]. Thus, we see a “real contrast” between the increase in the supply of doctors and nurses, and its recruitment (demand) by the NHS, although there might be “nuances” to this interpretation, as detailed in what follows (Figure 5.2).
We highlight the negative evolution of nurse recruitment; however, with respect to doctors, the increase is a result of the enrollment of young people in training programs and with short term contracts, being still necessary to refer to certain clinical expertise where Portuguese NHS shows a deficit in qualified HHR.
We understand this growth as unreal, and it coincides with the exit of doctors from the NHS (due to, for example, retirement or emigration), which is why the perspective of “quality gains” in terms of assistance and training capacity is, indeed, negative (Figures 5.3, 5.4, and Table 5.1) [22, p. 29].
The percentage of NHS doctors and nurses who work on basic health care is half that who work in hospitals or in other health-related services, based on data from 2000 to 2007; the number of other health professionals in this field increased during the same period [20].
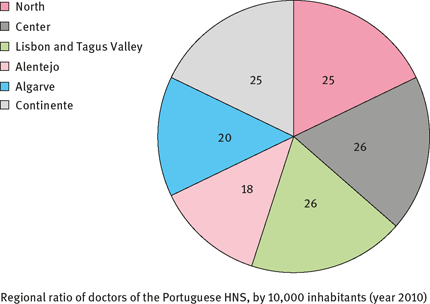
HHR assignments are based on two criteria: the greater distance of the three more desired geographical areas and the population density of the geographical areas covered. However, these criteria appear to be obsolete, as “they have been contributing to the regional differences of assignment,” given the covered population [19, pp. 4–5]. Confirming the situation, we see that the coverage ratio of NHS doctors for every 10,000 inhabitants ranges from 26 in the Lisbon Tagus Valley and central region and 18 in the Alentejo region (Table 5.2 and Figure 5.5) [22].
To overcome the shortage of specialized (expert) health professionals, particularly in certain clinical specialties (areas of expertise), the Ministry of Health imports equivalent foreign HHR as an easy way to solve this problem (Figure 5.6). Nonetheless, Portuguese nationals predominate in the NHS, representing more than 93% of the total, an increase over the 2009 level [22].
With respect to HHR management, the importance of the link “Indefinite Labor Contract in Public Functions” diminished between 2005 and 2010 in terms of the evolution of the forms of contractual ties predominant in the Portuguese NHS, reflecting legislative changes in public administration recruitment (Figures 5.5 and 5.7). In addition, the number of people working between 35 and 42 hours also dropped, while the number of those working 40 hours increased [22].
According to the same source, we verify that the NHS covers the country offering its services according to the two major health subregions, in line with the major national metropolitan areas (Oporto and Lisbon), with more than 40 healthy centers, organized according to geographical area. These integrate more than 100 health extensions, with a total equivalent to thousands of HHR depending on ministry directives. The management of HHR in the Portuguese NHS is vertically integrated and, hence, largely dependent on those in power at a given time. New laws governing hospital management and the network of primary health care centers underline the constraints that this situation could impose on the implementation of SHRM in the Portuguese NHS since they reflect the Ministry of Health’s monopolist role in the appointments of hospital and health center directors. This idea relate to that of the last paragraph, showing and emphasizing the Ministry of Health’s primary role in the management of the NHS’s activities, which is also reflected in the approval of hospitals’ activities, which are developed by the ministry, even though such activities could be overseen by the various health regions [24]. This centralization smakes impossible and is contrary to the structure of SHRM in the Portuguese NHS.

Table 5.1: Growth rate in total number of clinics, according to clinical expertise, in Portuguese NHS (comparison 2002–2011). (Source: Adapted from [22]).
| Career | Specialty | Growth (2002/2011) |
| Hospital | 8% | |
| Pathological Anatomy | −18% | |
| Anesthesiology | 26% | |
| Cardiology | 11% | |
| Pediatric Cardiology | 16% | |
| Cardiothoracic Surgery | −1% | |
| General Surgery | 12% | |
| Maxillofacial Surgery | 7% | |
| Pediatric Surgery | 22% | |
| Plastic Surgery | −1% | |
| Vascular Surgery | 26% | |
| Dermatology | −10% | |
| Endocrinology | 0% | |
| Estomatology | −19% | |
| Gastroenterology | 5% | |
| Medical Genetics | 50% | |
| Gynecology/Obstetrics | −11% | |
| Clinical Hematology | 4% | |
| Immunoallergology | 54% | |
| Immunohemotherapy | −3% | |
| Infectiology | 54% | |
| Physical Medicine/Rehabilitation | 3% | |
| Internal Medicine | 26% | |
| Nuclear Medicine | 6% | |
| Nephrology | 40% | |
| Neurosurgery | 4% | |
| Neurology | 19% | |
| Neurocardiology | 56% | |
| Ophthalmology | −4% | |
| Medical Oncology | 231% | |
| Orthopedics | −3% | |
| Otolaryngology | −1% | |
| Clinical Pathology | −12% | |
| Medical Pediatrics | 9% | |
| Pedopsychiatry | 34% | |
| Pneumology | 15% | |
| Psychiatry | −18% | |
| Radiology | 7% | |
| Radiotherapy | −19% | |
| Rheumatology | 63% | |
| Urology | 5% | |
| General Clinic | General/Family Medicine No Specialty – General Clinic |
−14% (Data not available) |
| Public Health | Public Health | −24% |
| Hospital Doctor | 36% | |
| Other | (Data not available) | |
| Atypical Categories | (Data not available) | |
| Total General | 9% |
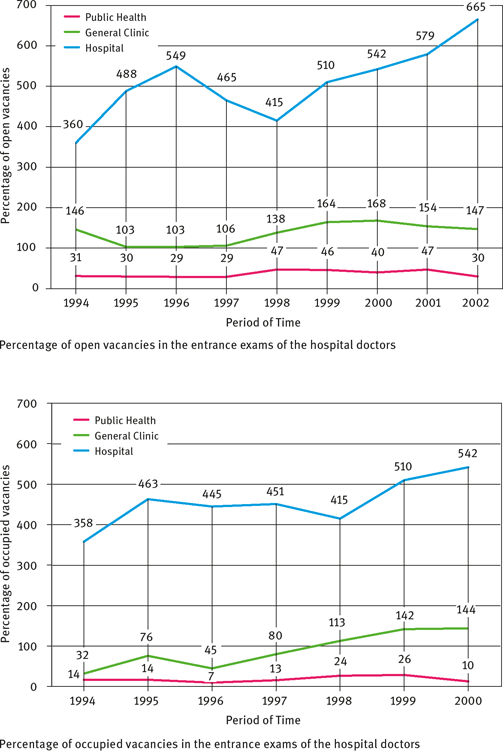
Table 5.2: Inhabitant ratio by specialist (expert) doctors in NHS, according to respective career and specialty (comparison 2002–2011). (Source: Adapted from [22]).




5.3.2Observed performance in HRM in Portuguese NHS compared with expected performance (SHRM), according to five Peretti vectors
With the collected data, we analyzed HR functions to draw conclusions about the performance of HHR in the Portuguese NHS in the period 2000–2010, at the level of the three work processes to achieve health aims, according to the adopted theoretical model and the aims established in this study. Because we believe that it will be possible for the Portuguese NHS to improve its organizational performance only when it adopts an SHRM model, we tried to verify, in the previously given description of such processes, the possibility of its orientation according to the five vectors of Peretti [16].
With regard to the process of competency development, we have observed a lack of SHRM in the Portuguese NHS, so continuous professional training presents constraints, in view of its quality and infrequency, as well as its inadequacy for the labor market and health needs. Looking at the particular case of migrant professionals, regulation on the recognition of foreigners’ qualifications is weak, and there are several mechanisms: faculties, a medical association (Order), the Ministry of Health, among others.
Considering the HHR distribution process, we highlight the actual emphasis in SHRM in the Portuguese NHS, as in the country one can observe several imbalances in HHR distribution, by type of institution, region, or occupational category, which translates into inadequate usage of scarce and expensive resources, limiting the population’s access to the corresponding service they need.
In the Portuguese NHS reality, with respect to the HHR management process, oversight of workers’ administrative tasks– recruitment, placement, reward management, license and pension administration, discipline, and promotion – is centralized at the Ministry of Health and only implemented by personnel units. The involvement of HHR units in the NHS dynamics is limited mainly to bureaucratic processing and, thus, they merely carry out the directives of higher-level bodies, performing routine clerical duties.
The working conditions of HHR in this public service still face constraints in connection with satisfying their own needs and objectives owing to job insecurity, lack of career plans, compensation, and infrastructure problems, which as a result compromise the success of health policies and practices.
Thus, given the description of the observed performance in HRM in the Portuguese NHS, we confirm Hypothesis 1 (H1) over H0 since the two hypotheses examined in this study are mutually exclusive. In this regard, we again assert the accuracy of the theoretical model developed to analyze the proposed problematic for this study since the empirical evidence confirms the theoretical postulates: NHS cannot achieve organizational efficiency, in terms of its HHR labor performance, because it cannot accommodate an SHRM model, resulting in certain weaknesses with respect to its workforce, which represents a threat to the long-term viability of this public service. Some of these issues were also addressed by the World Health Organization in an evaluation report of the Portuguese National Health Plan, focusing on the situation of HHR in the Portuguese NHS [1].
To confirm such a conclusion, we explain in what follows why it is not possible to establish SHRM in the Portuguese NHS, supporting the conclusions of Dussault and Souza [20] in terms of the three processes mentioned earlier, taking into account the mistrust by the government, focusing on Peretti [16] vectors. This can be seen as an impulse to the competent authorities design and implement strategic HRM policies and practices in this service, which could be guided by the need to overcome the weak performance observed in each vector.
Regarding adaptation, awareness of NHS-specific issues is essential to implementing effective and strategic HRM policies and practices. Its structural renovation will not be enough to undertake effective revitalization initiatives. This will only be achieved by adjusting HHR skills in the organizational strategy. The particular features of the NHS are at the root of its problems, in particular with respect to “democracy and autonomy,” as the main mechanism of coordination (skills standardization, delegated in a central way according the directives of the Ministry of Health) will not be enough to meet all coordination needs, either from professionals among themselves or from them in the support sector. In terms of results, concerning this vector, the reflection of Lengnick-Hall, Beck and Lengnick-Hall [6] is pertinent, as we have established that the Portuguese NHS will be able to achieve resilience only by instituting an SHRM paradigm that will enable it to be more competitive in the current complex international environment, a result of globalization.
Regarding mobilization, the Portuguese NHS generally had no clear targets or instructions about HR performance appraisal and was unable to develop, in a systematic way, the respective health services. The careers of doctors and nurses are the only feature that has guaranteed, until now, mechanisms that aim at the evolution of their professionals toward high standards of accountability and compensation, which acts as a control mechanism by the Ministry of Health, as they permit a degree of hierarchy among such professionals [25]. We see in the NHS the proliferation of individual employment contracts, bringing disruption to labor perspectives and job insecurity, which erode values in this public service [25]. In this discussion, we base our interpretation on Huselid, Jackson and Schuler’s [2, p. 174] reflections, which address the existence of certain business-related capacities, in addition to techniques that foster the adoption of an SHRM paradigm because of the perception that technical capacities are not enough to ensure an effective HRM standard. Such business-related capacities would allow workers to understand how unique considerations relative to their organization’s activities could create in itself HRM-specific needs.
Regarding customization, the monthly salary remains the base of HHR compensation in the Portuguese NHS; however, overtime, which are customary and regular, are also a significant part of compensation. According to SHRM, beyond the monthly salary other incentives should be included, like access to or support for training, leaves of absence, flextime, or sabbaticals. These are under discussion in the government,14but a lack of knowledge about how to formally appraise the current situation and any kind of cohesive and coherent reflection among professionals and their representatives regarding performance measurement in the different activity areas makes its implementation difficult. In this discussion we follow Huselid, Jackson and Schuler [2] in suggesting the need for specific activities in the implementation of a competitive strategy in organizations and in the achievement of their operational objectives. However, there exists a poor understanding about how to reach its effective implementation, having few guides, not existing, a customization in such activities. Therefore, we expect that such HRM strategic activities are relatively few, as is attested by the actual performance characteristics of the Portuguese NHS.
With regard to sharing, the Ministry of Health has monopoly control over NHS strategies, which ensure that HHR act simply as its executors. In contrast, in an SHRM paradigm, HRM strategy establishment and execution should be formulated in cooperation with workers in a dynamic of reciprocal interaction and collaboration among the parties. Only in this way will the HHR of the Portuguese NHS be able to act as agents of continuous change. There is a problem with myopia, as the organizational vision of the Portuguese NHS is not shared among all its components. Theoretical grounds that we have used in the discussion of the results achieved in the interpretation of the vectors mobilization and customization are also relevant for this vector interpretation.
Analyzing the anticipation vector, we have observed that many entities collect information about HHR in Portugal, according to different criteria. To make things worse, NHS data are not always published in a timely manner, making it difficult to share and access information for a coherent and integrated data analysis. There is also a lack of confidence in the intellectual capital of the Portuguese NHS, as the evolution of this public service is mainly the result of normative initiatives, of a “top-down” logic in terms of power, with little participation from civil society and the HHR who operate the system. Thus, it is difficult to map solutions to anticipate and respond efficiently to challenges that might arise from changes in circumstances in the health environment. On theoretical grounds, the discussion on this Peretti vector is similar to that of the adaptation vector.
Conclusion
There is not a clear HHR policy or a HRM strategy in the Portuguese NHS that would justify the inefficient organizational performance in this public sector, corroborating previous studies [18]. NHS evolution aims to preserve a public service culture clearly differentiated and qualified, but the maintenance and elevation of this standard require investing in HHR. SHRMhas emerged as a bold answer, as it is based on another type of psychological and social contract, valuing human capital and new forms of relationships with workers.
HRM practice is not neutral as it reflects the values of one organization and its search for objectives related to the adopted values. We argue that the problem that makes impossible SHRM in the Portuguese NHS lies in the myopia of current policies, mainly those of the Ministry of Health, the system’s main overseer, because it focuses on an administrative and bureaucratic standard, motivated solely by cost savings.
The conclusions drawn here align with findings in the literature on emergent tendencies that focus on strategy, which is why we share Becker and Huselid’s [12] point of view, as we argue that the current theory should expand to focus on the effective implementation of a strategy in the key variables of mediation between HR architecture and achieving organizational performance, and in this way, the organization will reach a level of differentiation, improving its performance.
This will be one of the more critical dimensions of analysis in the SHRM sphere once it looks to determine the best way to evolve so as to improve its operational efficiency to bring about the transformation of its practices and establish sustainable competitive advantages for the organization.
This work outlines directions for future research that will be critical for developing mediation tools. Thus, based on the study presented in this chapter, it is vital to stimulate more systematic work on the relationship between quality standards for individual work units and the organization as a whole. It is therefore of the utmost importance to stress a combination of three axes: performance practices in use in a unit, the identification of areas of improvement should be made, and the individual and team education needs. In this way, it will be possible to attain team commitment, at the individual and collective levels, as HHR in the Portuguese NHS will recognize their contribution to improving services. This is the main recommendation that this study makes for the development of SHRM in the Portuguese NHS, which is why legal mechanisms for its implementation and monitoring, and HHR performance appraisal models, will be topics of future research, on the basis of the various gaps presented in each of Peretti’s vectors, as indicated in our description of the observed performance in the Portuguese NHS.
This work also presents limitations, primarily owing to a scarcity of information on this topic and to the difficulty of accessing the available information (a result of the fact that this information is usually collected and interpreted by many entities, according to different criteria, which makes it difficult to analyze). Indeed, it was not always possible to meet all of our research goals with respect to the chosen period of analysis, which made it impracticable to make comparisons and formulate standards on the evolution, in the same circumstances, of certain factors. Thus, the topics covered in this study may be investigated in greater depth in future research.
Bibliography
[1]Organização Mundial de Saúde, departamento regional para a Europa (2009). Evaluation of National Health Plan of Portugal (2004–2010). Copenhaga: Publicações da OMS. Accessed in 10 October 2015, at http://www.acs.min-saude.pt/files/2010/03/WHO-Evaluation-NHP-Final-March16.pdf.
[2]Huselid M, Jackson S, Schuler R (1997). Technical and Strategic Human Resource Management Effectiveness as Determinants of Firm Performance. The Academy of Management Journal 40(1):171–188.
[3]Wright P, McMahan G (2011). Exploring human capital: putting human back into strategic human resource management. Human Resource Management Journal 21(2):93–104.
[4]Combs JG, Liu Y, Hall AT, Ketchen DJ (2006). Do high performance work practices matter? A meta-analysis of their effects on organizational performance. Personnel Psychology 59(3):501– 528.
[5]Lengnick-Hall C, Lengnick-Hall M (1988). Strategic Human Resources Management: A Review of the Literature and a Proposed Typology. The Academy of Management Review 13(3):454–470.
[6]Lengnick-Hall C, Beck T, Lengnick-Hall M (2011). Developing a Capacity for Organizational Resilience Through Strategic Human Resource Management. Human Resource Management Review 21:243–255.
[7]Wright P, Dunford B, Snell S (2001). Human resource and the resource based view of the firm. Journal of Management 27(1):701–721.
[8]Ulrich D (1998). A New mandate for human resources. Harvard Business Review, January– February, 124–135.
[9]Pfeffer J (1994). Competitve Advantage through people. Boston: Harvard Business School Press.
[10]Huselid M, Becker B (2011). Bridging Micro and Macro Domains: Workforce Differentiation and Strategic. Journal of Management 37(2):421–428.
[11]Jamrog J, Overholt M (2004). Building a Strategic HR Function: Continuing the Evolution. Human Resource Planning 27(1):51–62.
[12]Huselid M, Becker B (2006). Strategic Human Resources Management: Where Do We Go From Here? Journal of Management 32(6):898–925.
[13]Wright P, McMahan G (1992). Theoretical perspetives for strategic human resource Management. Journal of Management 18(2):295–320.
[14]Tavares S, Caetano A (1999). A emergência da Gestão de Recursos Humanos Estratégica. In Caetano A (coord), Mudança Organizacional e Gestão de Recursos Humanos. Lisboa: Observatório do Emprego e Formação Profissional.
[15]Prahalad CK, Hamel G (1990). The Core Competence of the Corporation, Harvard Business Review 90(3):79–91.
[16]Peretti J-M (1998). Recursos Humanos. 2nd edn. Lisboa: Sílabo.
[17]Dussault G, Souza L (1999). Gestão de Recursos Humanos em Saúde. Canadá: Universidade de Montreal.
[18]Biscaia A, Conceição C, Martins J, Ferrinho P (2003). Política e Gestão dos Recursos Humanos na Saúde em Portugal – Controvérsias. Revista Portuguesa de Clínica Geral 19:281–289.
[19]Gregório J, Lapão L (2003). Uso de cenários estratégicos para planeamento de recursos humanos em saúde: o caso dos farmacêuticos comunitários em Portugal 2010–2020. Revista Portuguesa de Saúde Pública 30(2):125–142.
[20]Dussault G, Fronteira I (2010). Recursos Humanos para a Saúde (RHS): Plano integrado no Plano Nacional de Saúde 2011–16 (PORTUGAL). Lisboa: Alto Comissariado da Saúde.
[21]Administração Central do Sistema de Saúde (2009). Estudo de necessidades previsionais de recursos humanos em saúde (médicos). Lisboa: ACSS.
[22]Santana P (coord) (2013). Estudo de Evolução Prospectiva de Médicos no Sistema Nacional de Saúde [Relatório Final]. Coimbra: Universidade de Coimbra.
[23]Observatório Português do Sistema de Saúde (OPSS) (2003). SAÚDE: que rupturas? Relatório de Primavera 2003. Lisboa: Escola Nacional de Saúde Pública.
[24]Decreto-Lei no. 19/88 (1988). Aprova a Lei de Gestão Hospitalar, Diário da República 1. Série, no. 248-(20) (21-01).
[25]Decreto-Lei no. 177/09 (2009). Regulamenta a carreira médica. Diário da República 1. série no. 149 (04-08).
[26]Decreto-Lei no. 117/98 (1998). Instituindo o Regime Remuneratório Experimental. Diário da República, 1. Série-A no. 103 (05-05).
[27]Rodrigues J, Biscaia L, Ministro L, Pisco L (1998). Monitorização da Qualidade Organizacional dos Centros de Saúde. Lisboa: Direcção Geral da Saúde.