
Chapter 25
ANAPLASMA, CHLAMYDOPHILA, COXIELLA, EHRLICHIA, and RICKETTSIA
Dennis J. Darcey*
Anaplasma, Coxiella, Ehrlichia, and Rickettsia spp. were previously considered as members of the same family but are now considered distinct entities based on genetic analysis. These groups of organisms are bacteria but only grow inside living cells.
ANAPLASMA
Common names for disease: Anaplasmosis, human granulocytic anaplasmosis (HGA), previously described as human granulocytic ehrlichiosis (HGE)
Occupational setting
Ranchers, farmers, foresters, rangers, hunters, lumberjacks, landscapers, outdoor workers, veterinarians, and research and laboratory technicians are at increased risk of exposure.
Exposure (route)
Anaplasma is transmitted to humans by the bite of an infected tick. The blacklegged tick (Ixodes scapularis) is the vector of Anaplasma phagocytophilum in the northeast and upper midwestern United States, and the western blacklegged tick (Ixodes pacificus) is the primary vector in Northern California (Figure 25.1).1 Cases have also been confirmed in several European and Asian countries.

FIGURE 25.1 Map of the United States showing the number of Anaplasma phagocytophilum cases by county in 2012. Cases are reported primarily from the upper Midwest and coastal New England, reflecting both the range of the primary tick vector species, Ixodes scapularis—also known to transmit Lyme disease and babesiosis—and the range of preferred animal hosts for tick feeding.
Source: MMWR 2015; 62(53):67.
Pathobiology
In the early 1990s, patients from Michigan and Wisconsin with a history of tick bites were described as having an illness similar to human monocytotropic ehrlichiosis but were notable for the presence of inclusion bodies in granulocytes rather than monocytes.2 The syndrome was initially called human granulocytic ehrlichiosis. The disease is now called human granulocytic anaplasmosis (HGA) after phylogenetic analysis reclassified Ehrlichia phagocytophilum as a member of the genus Anaplasma.2
Anaplasma phagocytophilum selectively inhabit and replicate within intracellular vacuoles of their host cells.2 They have an ultrastructural similarity to gram-negative bacteria but lack a lipopolysaccharide endotoxin.3
The symptoms caused by infection with A. phagocytophilum usually develop 1–2 weeks after being bitten by an infected tick. The tick bite is usually painless, and about half of the people who develop anaplasmosis may not recall being bitten by a tick. Symptoms vary from mild to severe, but common presentations include fever, headache, confusion, cough, chills, malaise, muscle pain, nausea, and abdominal pain.1 Rash is seen in less than 10% of patients with anaplasmosis3 and may indicate coinfection with Borrelia burgdorferi and/or Rickettsia rickettsii.
Most patients develop transient reductions in white cell and platelet counts. Relative granulocytosis with a left shift and lymphopenia is common during the first week of illness.4 During the acute phase, serum hepatic transaminase concentrations usually increase two- to fourfold, and inflammatory markers, such as C-reactive protein and the erythrocyte sedimentation rate, are increased.4 Deaths do occur but are rare. Persons with compromised immunity caused by immunosuppressive therapies (such as corticosteroids, chemotherapy, or immunosuppressive therapy following organ transplant), HIV infection, or splenectomy appear to develop more severe disease and may also have higher case fatality rates.1
Diagnosis
The incidence of infection is highest in the United States during the summer months when human tick encounters are at their peak with increased outdoor activities. The diagnosis of anaplasmosis is made based on clinical signs and symptoms consistent with the disease and history of tick bite, illness in an area where ticks are known to be present, or recent travel to an area where anaplasmosis is endemic. Early treatment is more likely to be effective and should be initiated if anaplasmosis is suspected.1 Treatment should not be delayed while awaiting laboratory test results, nor should it be withheld or withdrawn on the basis of an initial negative laboratory test result.1
Cytoplasmic inclusion bodies (morulae) are seen on a peripheral blood smear in 25–75% of cases and can aid in early diagnosis (Figure 25.2).2
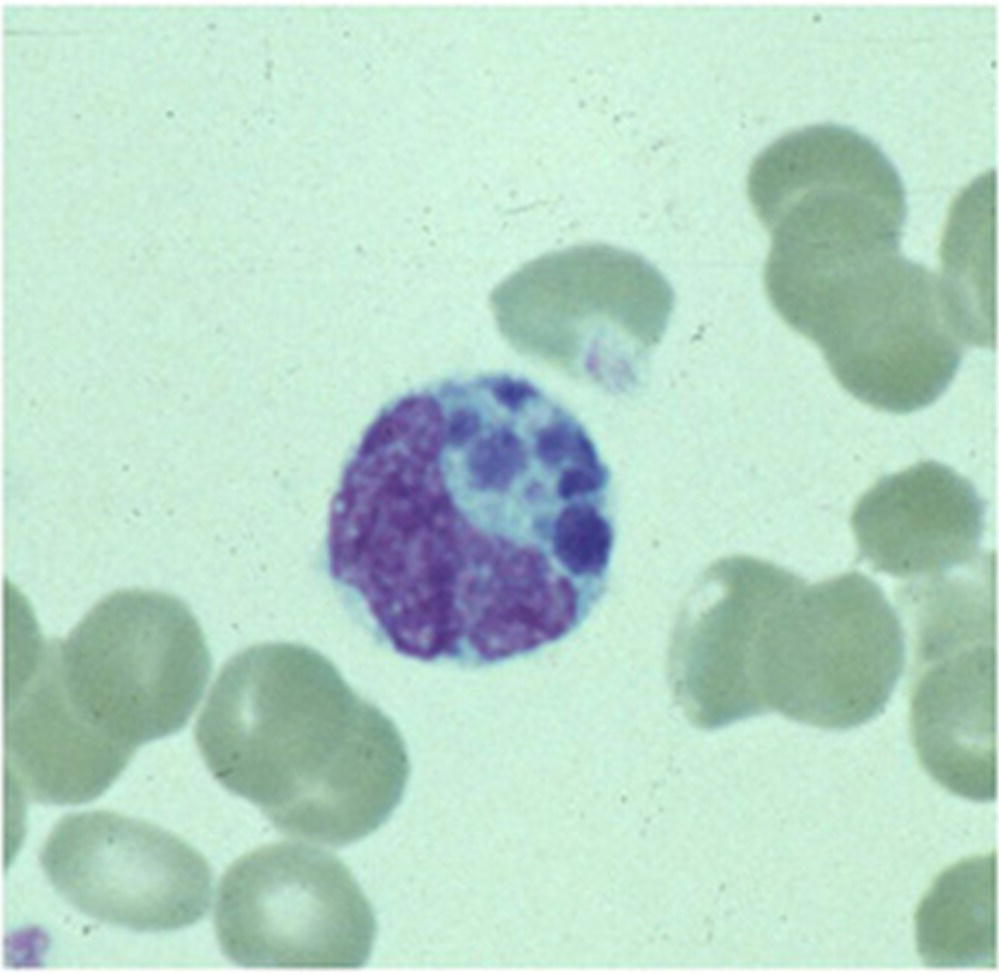
FIGURE 25.2 Morulae detected in a granulocyte on a peripheral blood smear, associated with A. phagocytophilum infection. .
Source: Centers for Disease Control and Prevention: Anaplasmosis, http://www.cdc.gov/anaplasmosis/symptoms/index.html
During the acute phase of illness, a sample of whole blood can be tested by polymerase chain reaction (PCR) assay to determine if a patient has anaplasmosis. This method is most sensitive in the first week of illness and quickly decreases in sensitivity following the administration of appropriate antibiotics. Although a positive PCR result is helpful, a negative result does not completely rule out the diagnosis.1 The gold standard serologic test for diagnosis of anaplasmosis is the indirect immunofluorescence assay (IFA) using A. phagocytophilum antigen, performed on paired serum samples to demonstrate a significant (fourfold) rise in antibody titers.1 The first sample should be taken as early in the disease as possible, preferably in the first week of symptoms, and the second sample should be taken 2–4 weeks later. In most cases of anaplasmosis, the first IgG IFA titer is typically low, or negative, and the second typically shows a significant (fourfold) increase in IgG antibody levels. IgM antibodies usually rise at the same time as IgG near the end of the first week of illness and remain elevated for months or longer. IgM antibodies are less specific than IgG antibodies and more likely to result in a false positive result. For these reasons, physicians requesting IgM serologic titers should also request a concurrent IgG titer.1
Serologic tests based on enzyme immunoassay (EIA) technology are available from some commercial laboratories. However, these tests are qualitative and less useful to measure changes in antibody titers between paired specimens. Some EIA assays rely on the evaluation of IgM antibody alone, which may have a higher frequency of false-positive results.1
Treatment
Doxycycline is the treatment of choice, and patients should be treated for 7–14 days or at least 3 days after defervescence.1 This treatment course will also treat the possibility of coinfection with B. burgdorferi (patients with coinfection should be treated for 14 days).4 Fever typically subsides within 24–48 hours after treatment when the patient receives doxycycline or another tetracycline during the first 4–5 days of illness.5 If a patient fails to respond to early treatment with a tetracycline antibiotic (i.e., within 48 hours), an alternate diagnosis should be considered.5 Recovery may be prolonged in severely ill patients.5
Medical surveillance
Routine medical surveillance is not recommended.
Prevention
To prevent infection from tick bites, avoid wooded and bushy areas with high grass. The use of tick repellants such as DEET (N,N-diethyl-3-methylbenzamide) on exposed skin and permethrin on clothing coupled with timely skin examination and removal of ticks after exposure to tick-infested environments can prevent infection. Antibiotic treatment is not recommended following a tick bite to prevent anaplasmosis.1 There are no licensed vaccines for anaplasmosis. In the laboratory, Anaplasma should be handled at biosafety level 2 (BSL2).6
References
- 1. Centers for Disease Control and Prevention. Anaplasmosis. http://www.cdc.gov/anaplasmosis/symptoms/index.html (accessed June 17, 2016).
- 2. Ismail N, Bloch KC, McBride JW. Human ehrlichiosis and anaplasmosis. Clin Lab Med 2010; 30(1):261–92.
- 3. Borjrsson DL, Barthold SW. The mouse as a model for investigation of human granulocytic ehrlichiosis: current knowledge and future directions. Comp Med 2002; 52(5):403–13.
- 4. Bakken JS, Dumler JS. Clinical diagnosis and treatment of human granulocytotropic anaplasmosis. Ann NY Acad Sci 2006; 1078:236–47.
- 5. Chapman AS, Backend JS, Folk SM, et al. Diagnosis and management of tickborne rickettsial diseases: rocky mountain spotted fever, ehrlichioses, and anaplasmosis—United States: a practical guide for physicians and other health-care and public health professionals. MMWR Recomm Rep 2006; 55(RR-4):1–27. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5504a1.htm (accessed on July 2, 2016).
- 6. Chosewood LC, Wilson DE, Centers for Disease Control and Prevention, National Institutes of Health. Biosafety in microbiological and biomedical laboratories, 5th edn. HHS publication no. (CDC) 21-1112, 2009. Washington, DC: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institutes of Health. Available at: http://www.cdc.gov/biosafety/publications/bmbl5/ (accessed on July 2, 2016).
CHLAMYDOPHILA PSITTACI
Common names for disease: Psittacosis, ornithosis, parrot fever, previously known as Chlamydia psittaci
Occupational setting
Bird handlers, pet shop workers, zoo attendants, poultry workers, laboratory personnel, veterinarians, and veterinary technicians are at risk from exposure.
Exposure (route)
Inhalation of secretions or excrement of infected domestic birds (parakeets, parrots, macaws, cockatiels, pigeons, turkeys, chickens, ducks, etc.) is the most common route of exposure. Person-to-person transmission has been reported, including infections in healthcare workers.1–3
Pathobiology
Chlamydophila psittaci (previously known as Chlamydia psittaci) is a gram-negative obligate intracellular bacterium. Once inhaled, C. psittaci rapidly enters the bloodstream and is transported to the reticuloendothelial cells of the liver and spleen. It replicates in these sites and then invades the lungs and other organs by hematogenous spread. The incubation period ranges from 5 to 15 days. Disease often starts abruptly and causes influenza type symptoms with chills, headache, malaise, and anorexia. Myalgias and arthralgias are common. A persistent dry hacking cough is prominent and complications can result in severe pneumonia. Respiratory symptoms are often mild compared to the extensive changes present on chest X-ray. Occasionally, changes in mentation may be noted. Hepatosplenomegaly may also occur in a significant number of patients. Myocarditis and encephalitis complications are rare but may occur.4 There are no characteristic laboratory or chest X-ray changes. Since 1996, fewer than 50 confirmed cases per year have been reported in the Unites States. Many more cases may occur that are not correctly diagnosed or reported.5
Diagnosis
The diagnosis can be confirmed either by isolation of the organism in culture or by serologic studies. Most diagnoses are established by clinical presentation and positive antibodies against C. psittaci in paired sera using microimmunofluorescence (MIF) methods. MIF is more sensitive and specific than the previously used complement fixation (CF) tests; however, there is still some cross-reactivity with other chlamydiae (Chlamydophila pneumoniae, Chlamydia trachomatis, and Chlamydophila felis) so a titer result less than 1 : 128 should be interpreted with caution. Acute-phase serum specimens should be obtained as soon as possible after the onset of symptoms, and convalescent-phase serum specimens should be obtained at least 2 weeks after the first specimen. Because antimicrobial treatment can delay or diminish the antibody response, a third serum sample 4–6 weeks after the acute sample might help confirm the diagnosis. Real-time polymerase chain reaction (rt-PCR) assays have been developed for use in the detection of C. psittaci in respiratory specimens. These assays can distinguish C. psittaci from other chlamydial species and identify different genotypes. Chlamydia psittaci can also be isolated from the patient’s sputum, pleural fluid, or clotted blood during acute illness and before treatment with antimicrobial agents; however, few laboratories perform cultures because of the technical difficulty and occupational health concerns.4
Treatment
Tetracycline antibiotics are the drugs of choice for C. psittaci infection in humans. Mild to moderate cases can be treated with oral doxycycline (100 milligrams every 12 hours) or tetracycline hydrochloride (500 milligrams every 6 hours) for a minimum of 10 days. Severely ill patients should be treated with intravenous (IV) doxycycline hyclate (4.4 mg/kg/day divided into two infusions, maximum 100 mg/dose). Antibiotic therapy should be continued for at least 10–14 days after fever abates. Most C. psittaci infections are responsive to antibiotics within 1–2 days; however, relapses can occur. Although in vivo efficacy has not been determined, macrolide antibiotics are considered the best alternative agents in patients for whom tetracyclines are contraindicated (e.g., children <8 years of age, pregnant women, and persons allergic to tetracyclines). Prophylactic antibiotics are not routinely administered after a suspected exposure to C. psittaci, but may be considered in some circumstances.4
Medical surveillance
Routine medical surveillance is not recommended. If cases can be linked to a source of exposure, then surveillance of the pet shop, aviary, farm, or healthcare setting should be undertaken. Infected birds should be treated or destroyed. The area where they are housed should be cleaned and disinfected.
Prevention
To prevent transmission of C. psittaci to humans and among bird populations, aviary and pet shop owners should follow specific control measures recommended by the National Association of State Public Health Veterinarians.4 When cleaning cages or handling potentially infected birds, caretakers should wear protective clothing, which includes gloves, eyewear, a disposable surgical cap, and an appropriately fitted respirator with N95 or higher rating. In addition, necropsies of potentially infected birds should be performed in a biological safety cabinet. The carcass should be moistened with detergent and water to prevent aerosolization of infectious particles during the procedure. Bird caretakers with respiratory or influenza-like symptoms should seek prompt medical attention and inform their healthcare provider about bird contact.
For healthcare workers treating patients with psittacosis, enhanced Respiratory Protection and isolation may be needed when caring for severely ill patients.3
In the laboratory, C. psittaci is considered as biosafety level 2 (BSL2) and animal biosafety level 3 (ABSL3).6 For procedures that have a high potential for aerosolization, it should be handled at biosafety level 3 (BSL3).6
There is currently no vaccine available to prevent psittacosis.
References
- 1. Hughes C, Maharg P, Rosario P, et al. Possible nosocomial transmission of psittacosis. Infect Control Hosp Epidemiol 1997; 18:165–168.
- 2. McGuigan CC, McIntyre PG, Templeton K. Psittacosis outbreak in Tayside, Scotland, December 2011 to February 2012. Euro Surveill 2012; 17(22):pii: 20186.
- 3. Wallensten A, Fredlund H, Runehagen A. Multiple human-to-human transmission from a severe case of psittacosis, Sweden, January–February 2013. Euro Surveill 2014; 19(42):pii: 20937. http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=20937 (accessed June 17, 2016).
- 4. National Association of State Public Health Veterinarians (NASPHV). Compendium of Measures to Control Chlamydophila psittaci Infection among Humans (Psittacosis) and Pet Birds (Avian Chlamydiosis), 2010. http://www.nasphv.org/Documents/Psittacosis.pdf (accessed June 17, 2016).
- 5. Centers for Disease Prevention and Control. Psittacosis. http://www.cdc.gov/pneumonia/atypical/psittacosis.html (accessed June 17, 2016).
- 6. Chosewood LC, Wilson DE, Centers for Disease Control and Prevention, National Institutes of Health. Biosafety in microbiological and biomedical laboratories, 5th edn. HHS publication no. (CDC) 21-1112, 2009. Washington, DC: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institutes of Health. Available at: http://www.cdc.gov/biosafety/publications/bmbl5/ (accessed on July 2, 2016).
COXIELLA BURNETII
Common name for disease: Q fever
Occupational setting
Q fever is a nationally notifiable disease caused by the bacterium Coxiella burnetii. The Centers for Disease Control and Prevention (CDC) receives approximately 150 reports of this illness in the United States each year (Figure 25.3). Occupations at risk include abattoir and livestock workers, dairy workers, veterinarians, veterinary and laboratory technicians, laboratory animal handlers, farmers, ranchers, and hide and wool handlers. Farmers who are in contact with cattle, sheep, and goats, assisting in the birthing of lambs, or exposed to birth by-products of other animals such as dogs and cats are at particularly high risk. Although Q fever has been historically considered an occupational disease, most cases reported to CDC each year involve individuals who do not report livestock contact and do not work with animals. These cases are likely due to airborne transmission of the bacteria after environmental contamination by infected animals.

FIGURE 25.3 Map of the United States and U.S. territories showing the number of acute and chronic Q fever cases in each state and territory in 2013. Q fever, caused by Coxiella burnetii, is reported throughout the United States. Human cases of Q fever most often result from contact with infected livestock, especially sheep, goats, and cattle. * Number of Q fever acute cases/number of Q fever chronic cases.
Source: MMWR 2015; 62(53):88.
Exposure (route)
Exposure occurs through inhalation of aerosolized particles or direct contact with infected animals, primarily cattle, sheep, or goats. Placentas from infected sheep are extremely infectious. In addition to domesticated livestock, a broad range of domestic and wild animals are natural hosts for C. burnetii, including horses, dogs, swine, pigeons, ducks, geese, turkeys, squirrels, deer, mice, cats, and rabbits. Exposure to C. burnetii in research laboratories and veterinary hospitals has resulted in large outbreaks of Q fever.1, 2 The largest known reported Q fever outbreak involved approximately 4000 human cases and occurred during 2007–2010 in the Netherlands. This outbreak was linked to dairy goat farms near densely populated areas and presumably involved human exposure via a wind-borne route.3
Approximately 200 cases of acute Q fever were reported in US military personnel who had been deployed to Iraq since 2003. Investigations of these cases linked illness to tick bites, sleeping in barns, and living near helicopter zones with environmental exposure resulting from helicopter-generated aerosols.4, 5
Pathobiology
Coxiella burnetii is an obligate intracellular bacterium that appears as a short pleomorphic gram-negative rod. Coxiella burnetii grows in the phagosomes of the cell. It is very resistant to inactivation and can survive in the environment for long periods of time in the spore stage. Coxiella burnetii is extremely infectious.
Frequently underreported and misdiagnosed, acute Q fever often resembles a nonspecific viral illness. Symptomatic acute Q fever, which occurs in approximately half of infected persons, is characterized by a wide variety of clinical signs and symptoms. Q fever usually presents as a mild respiratory illness and is often described as one of the atypical pneumonias. The incubation period typically ranges from 2 to 3 weeks. Clinical signs and symptoms include fever, malaise, headache, weakness, and transient pneumonitis with cough, chest pain, myalgias, and arthralgias. Physical examination is often unremarkable, and the most common physical finding is inspiratory crackles. Fever lasts a median of 10 days in untreated patients but when treated fever defervesces within 72 hours of antibiotic administration. The majority of infections are mild and self-limiting. Although mortality is <2% in patients with acute Q fever, in the Netherlands outbreak, which included approximately 4000 reported cases, up to 50% of acute Q fever patients were hospitalized.6 Q fever infections in women that occur shortly before conception or during pregnancy increase the risk for miscarriage, stillbirth, premature birth, intrauterine growth retardation, and low birth weight. Less frequently described clinical symptoms include pericarditis, myocarditis, aseptic meningitis, encephalitis, and cholecystitis.
Chronic Q fever is rare, occurring in <5% of persons with acute infection with onset as soon as months, or as late as decades following an acute illness. The patients at highest risk for chronic Q fever are those with valvular heart disease, a vascular graft, or an arterial aneurysm.
Diagnosis
The diagnosis of Q fever can be made by isolating the organism in the laboratory or by serologic demonstration of infection. The most common serologic tests include complement fixation (CF) and indirect fluorescent (IFA) antibody procedures.
Seroconversion typically occurs 7–15 days after symptoms appear, and 90% of patients seroconvert by the third week of illness.7 In acute infection, a phase II IgG antibody is higher than the antibody response to phase I. The reverse is true in chronic infection. The most commonly used means of confirming the diagnosis of acute Q fever is demonstration of a fourfold rise in phase II IgG by IFA between serum samples from the acute and convalescent phases taken 3–6 weeks apart. However, IFA antibody results are not usually helpful in guiding immediate treatment decisions.
Treatment
Treatment for acute illness should begin immediately and not be delayed while awaiting laboratory results. The treatment of choice for acute Q fever is a 2-week course of doxycycline. Alternative regimens for specific groups of patients (e.g., pregnant women) and for chronic infection are discussed in detail within the complete Recommendations from CDC and the Q Fever Working Group.7 Management of chronic Q fever requires long-term treatment with multiple antibiotics and intensive patient monitoring for years for possible relapse. Surgical intervention may be required, and consultation with an infectious disease specialist is recommended.
Medical surveillance
Routine medical surveillance is not recommended.
Prevention
Coxiella burnetii organisms are widespread in the environment and resistant to inactivation. Control of major animal reservoirs of the organism is impractical. Personal protective equipment when handling affected animals, bedding, and their by-products and respiratory protection when working in dusty environments contaminated with organisms are recommended. Other preventive measures include pasteurization of milk to reduce the potential risk for transmission through milk and cheese products. Workers with prosthetic heart valves and liver disease are at particularly high risk for the sequelae of infection and are best restricted from high-risk environments. Biosafety level 2 (BSL2) practices, containment equipment, and facilities are recommended for nonpropagative laboratory procedures, including serological examinations and staining of impression smears. Biosafety level 3 (BSL3) practices and facilities are recommended for activities involving the inoculation, incubation, and harvesting of embryonated eggs or tissue cultures, the necropsy of infected animals, and the manipulation of infected tissues. Experimentally infected rodents should also be maintained under animal biosafety level 3 (ABSL3).8 Laboratory safety and containment recommendations for C. burnetii should be followed as described in the CDC Biosafety in Microbiological and Biomedical Laboratories Manual 5th edition8 and following the guidelines in Diagnosis and Management of Q Fever—United States: Recommendations from CDC and the Q Fever Working Group.7 Q fever is a nationally notifiable disease in the United States. Healthcare providers should report suspected or confirmed cases through local or state reporting mechanisms in place for notifiable disease conditions.
References
- 1. Johnson JE II, Kadull PJ. Laboratory-acquired Q fever. Am J Med 1966; 41:391–403.
- 2. Hall CJ, Richmond SJ, Caul EO, et al. Laboratory outbreak of Q fever acquired from sheep. Lancet 1982; 1:1004–6.
- 3. Schimmer B, Dijkstra F, Velllema P, et al. Sustained intensive transmission of Q fever in the south of the Netherlands, 2009. Euro Surveill 2009; 14:3.
- 4. Anderson AD, Baker TR, Littrell AC, et al. Seroepidemiologic survey for Coxiella burnetii among hospitalized U.S. troops deployed to Iraq. Zoonoses Public Health 2011; 58:276–83.
- 5. Faix DJ, Harrison DJ, Riddle MS, et al. Outbreak of Q fever among U.S. military in western Iraq, June–July 2005. Clin Infect Dis 2008; 46:e65–8.
- 6. Van der Hoek W, Dijkstra F, Schimmer B, et al. Q fever in the Netherlands: an update on the epidemiology and control measures. Euro Surveill 2010; 15:pii: 19520. Available at: http://www.eurosurveillance.org/ViewArticle.aspx?ArticleId=19520 (accessed on July 2, 2016)
- 7. Anderson A, Bijlmer H, Fournier PE, et al. Diagnosis and management of Q fever—United States: recommendations from CDC and the Q Fever Working Group. MMWR Recomm Rep 2013; 62(RR-3):1–30. Available at: https://www.cdc.gov/mmwr/preview/mmwrhtml/rr6203a1.htm (accessed on July 3, 2016).
- 8. Chosewood LC, Wilson DE, Centers for Disease Control and Prevention, National Institutes of Health. Biosafety in microbiological and biomedical laboratories, 5th edn. HHS publication no. (CDC) 21-1112, 2009. Washington, DC: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institutes of Health. Available at: http://www.cdc.gov/biosafety/publications/bmbl5/ (accessed on July 2, 2016).
EHRLICHIA SPECIES
Common name for disease: Ehrlichiosis, when caused by Ehrlichia chaffeensis, is also described as human monocytic ehrlichiosis (HME); infection with Ehrlichia ewingii is sometimes referred to as human ehrlichiosis ewingii (HEE).
Occupational setting
Ranchers, farmers, foresters, rangers, hunters, lumberjacks, landscapers, outdoor workers, veterinarians, and research and laboratory technicians are at increased risk of exposure.
Exposure (route)
Ehrlichia chaffeensis and Ehrlichia ewingii are transmitted by the lone star tick in the southeastern and south central United States (Figures 25.4 and 25.5). In addition, a third Ehrlichia species provisionally called Ehrlichia muris-like (EML) has been identified in a small number of patients residing in or traveling to Minnesota and Wisconsin; a tick vector for the EML organism has not yet been established.1
FIGURE 25.4 Map of the United States showing the number of Ehrlichiosis (Ehrlichia chaffeensis) cases by county in 2013. E. chaffeensis is the most common type of ehrlichiosis infection in the United States. This tick-borne pathogen is transmitted by Amblyomma americanum, the lonestar tick, whose geographic range extends from the Southeast into parts of the Northeast and Midwest. The majority of cases of E. chaffeensis are reported from the Midwest, South, and Northeast regions. .
Source: MMWR 2015; 62(53):64
FIGURE 25.5 Map of the United States that presents the number of Ehrlichiosis (Ehrlichia ewingii) cases in by county in 2013. Ehrlichiosis ewingii is the least common cause of ehrlichiosis. E. ewingii is carried by Amblyomma americanum, the lonestar tick, which is the same vector that transmits E. chaffeensis. Currently, no serologic tests are used to distinguish between the two species, and differentiation can only be made by molecular genotyping. .
Source: MMWR 2015; 62(53):53
Pathobiology
Ehrlichiae are obligate intracellular bacteria that grow within membrane-bound endosomes in human and animal phagocytic or endothelial cells and establish persistent infection in their vertebrate reservoir hosts.2 Previously, Ehrlichiae were divided into human monocytic ehrlichiosis (HME) and granulocytic ehrlichiosis (HGE). However, the causative organism for infection of granulocytes has been reclassified and is now called A. phagocytophilum, and the disease is termed anaplasmosis or human granulocytic anaplasmosis (HGA) and is discussed in the section on “Anaplasma” at the beginning of this chapter.
Ehrlichia ewingii was considered to be exclusively a canine pathogen until the first human cases of infection were described in 1999. Most infections reported to date have occurred in patients with HIV or who were immunosuppressed following organ transplantation.3 Although the infection occurs in immunocompromised patients, symptoms have generally been milder with E. ewingii.3
The symptoms caused by infection with these Ehrlichia species usually develop 1–2 weeks after being bitten by an infected tick. The tick bite is usually painless, and about half of the people who develop ehrlichiosis may not remember being bitten by a tick. Symptoms vary from mild to severe, but common presentations include fever, meningitis, meningoencephalitis, headache, chills, malaise, muscle pain, nausea, vomiting, diarrhea, confusion, conjunctival injection, and rash (in up to 60% of children, less than 30% of adults).1
About 40% of those with E. chaffeensis infection require hospitalization.3 Severe infections may resemble toxic shock syndrome or Rocky Mountain spotted fever.3
Laboratory findings may include hyponatremia, thrombocytopenia, leucopenia, anemia, and elevated aminotransferase levels. For patients that undergo lumbar puncture, the CSF WBC count is typically <100 cells/mm3 and protein may be mildly elevated.3
Deaths do occur but are rare. Persons with compromised immunity caused by immunosuppressive therapies (such as corticosteroids, chemotherapy, or immunosuppressive therapy following organ transplant), HIV infection, or splenectomy appear to develop more severe disease with E. chaffeensis and may have higher case fatality rates.
Diagnosis
The incidence of infection is highest in the United States during the summer months when human tick encounters are at their peak with increased outdoor activities. The diagnosis of ehrlichiosis is made based on clinical signs and symptoms consistent with the disease and history of tick bite, illness in an area where ticks are known to be present, or recent travel to an area where ehrlichiosis is endemic. Treatment should never be delayed pending the receipt of laboratory test results or be withheld on the basis of an initial negative laboratory result.
Cytoplasmic inclusion bodies (morulae) are seen on a peripheral blood smear in up to 20% of cases and can aid in early diagnosis (Figure 25.6).1 Ehrlichia chaffeensis usually infects monocytes, while E. ewingii more commonly infects granulocytes.1 However, morulae in a particular cell type cannot conclusively identify the infecting species.1 Routine hospital blood cultures cannot detect Ehrlichia.1
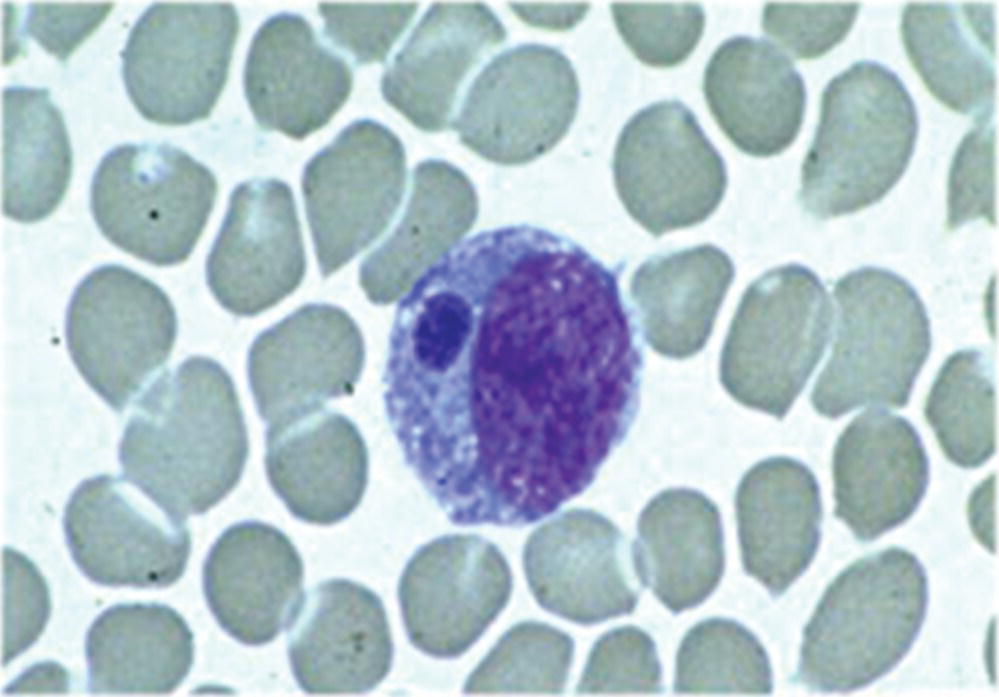
FIGURE 25.6 Morulae detected in a monocyte on a peripheral blood smear, associated with E. chaffeensis infection.
Source: Centers for Disease Control and Prevention: Ehrlichiosis. http://www.cdc.gov/ehrlichiosis/symptoms/index.html
During the acute phase of illness, a sample of whole blood can be tested by polymerase chain reaction (PCR) assay to determine if a patient has ehrlichiosis. This method is most sensitive in the first week of illness and quickly decreases in sensitivity following the administration of appropriate antibiotics. Although a positive PCR result is helpful, a negative result does not completely rule out the diagnosis.1 The gold standard serologic test for diagnosis of ehrlichiosis is the indirect immunofluorescence assay (IFA) using E. chaffeensis antigen, performed on paired serum samples to demonstrate a significant (fourfold) rise in antibody titers. The first sample should be taken as early in the disease as possible, preferably in the first week of symptoms, and the second sample should be taken 2–4 weeks later. In most cases of ehrlichiosis, the first IgG IFA titer is typically low, or “negative,” and the second typically shows a significant (fourfold) increase in IgG antibody levels. IgM antibodies usually rise at the same time as IgG near the end of the first week of illness and remain elevated for months or longer. IgM antibodies are less specific than IgG antibodies and more likely to result in a false positive. For these reasons, physicians requesting IgM serologic titers should also request a concurrent IgG titer.1
Serologic tests based on enzyme immunoassay (EIA) technology are available from some commercial laboratories. However, these tests are qualitative and less useful to measure changes in antibody titers between paired specimens. Some EIA assays rely on the evaluation of only IgM antibodies, which may have a higher frequency of false-positive results.1
Treatment
Doxycycline is the treatment of choice and patients should be treated for at least 10 days or for 3–5 days after defervescence.3 This treatment course will also treat the possibility of coinfection with B. burgdorferi and/or R. rickettsii. Fever typically subsides within 24–48 hours after treatment when the patient receives doxycycline or another tetracycline during the first 4–5 days of illness.3 If a patient fails to respond to early treatment with a tetracycline antibiotic (i.e., within 48 hours), an alternate diagnosis should be considered.4 Recovery may be prolonged in severely ill patients.4
Prevention
To prevent infection from tick bites, avoid wooded and bushy areas with high grass. The use of tick repellants such as DEET (N,N-diethyl-3-methylbenzamide) on exposed skin and permethrin on clothing coupled with timely skin examination and removal of ticks after exposure to tick-infested environments can prevent infection. Antibiotic treatment is not recommended following a tick bite to prevent ehrlichiosis.1
There are no licensed vaccines for ehrlichiosis or anaplasmosis. In the laboratory, Ehrlichia should be handled at biosafety level 2.5
References
- 1. Centers for Disease Control and Prevention. Ehrlichiosis. http://www.cdc.gov/ehrlichiosis/symptoms/index.html (accessed June 17, 2016).
- 2. Walker DH, Ismail N, Olano JP, et al. Ehrlichia chaffeensis: a prevalent, life-threatening, emerging pathogen. Trans Am Clin Climatol Assoc 2004; 115:375–382.
- 3. Ismail N, Bloch KC, McBride JW. Human Ehrlichiosis and Anaplasmosis. Clin Lab Med 2010; 30(1):261–292.
- 4. Chapman AS, Backend JS, Folk SM, et al. Diagnosis and management of tickborne rickettsial diseases: rocky mountain spotted fever, ehrlichioses, and anaplasmosis—United States: a practical guide for physicians and other health-care and public health professionals. MMWR Recomm Rep 2006; 55(RR-4):1–27. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5504a1.htm (accessed on July 2, 2016).
- 5. Chosewood LC, Wilson DE, Centers for Disease Control and Prevention, National Institutes of Health. Biosafety in microbiological and biomedical laboratories, 5th edn. HHS publication no. (CDC) 21-1112, 2009. Washington, DC: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institutes of Health. Available at: http://www.cdc.gov/biosafety/publications/bmbl5/ (accessed on July 2, 2016).
RICKETTSIA RICKETTSII
Common name for disease: Rocky Mountain spotted fever (RMSF)
In addition to Rickettsia rickettsii, other tick-borne species of Rickettsia, broadly grouped under the heading “Spotted Fever Group Rickettsia” (SFGR), have been shown to cause human infections. Tick-borne SFGR are transmitted to humans by the bite of an infected tick and may cause similar signs and symptoms to those observed for Rocky Mountain spotted fever (RMSF). These pathogens include several species of Rickettsia found in the United States, including R. parkeri and Rickettsia species 364D.
Occupational setting
Persons in outdoor occupations, including farming, forestry, landscaping, logging, construction, telephone lineman, environmental technicians, and some laboratory workers, are at risk from exposure.
Exposure (route)
Transmission of infection occurs primarily following bites from infected ticks or from skin contamination with tick tissue or feces when removing ticks from humans or animals, especially when the tick is crushed between the fingers. In the United States, these include the American dog tick (Dermacentor variabilis), Rocky Mountain wood tick (Dermacentor andersoni), and brown dog tick (Rhipicephalus sanguineus). The American dog tick, D. variabilis, is the most prevalent vector in the Eastern United States. The Rocky Mountain wood tick, D. andersoni, is the prevalent vector in the Western United States. Transmission of infection occurs after about 6–10 hours of feeding. There have also infections associated with needlestick injuries, blood transfusions, and among laboratory workers handling rickettsiae. Laboratory-acquired infection has also occurred following exposure to infectious aerosols.1
Pathobiology
Rickettsia rickettsii belongs to the spotted fever group of rickettsiae that are genetically related but different in their surface antigenic proteins. The Rickettsia is small obligate intracellular bacteria measuring approximately 0.3 to 1.0 microns in size. The cell wall has an ultrastructural appearance of a gram-negative bacterium and contains lipopolysaccharide (LPS).2 The LPS contains immunogenic antigens that are shared among the Rickettsia and cross-react with Proteus and Legionella. Cross-reactivity with Proteus is the basis for the Weil–Felix diagnostic test.
First recognized in the Rocky Mountain region, cases have been reported in almost every state. The incidence of disease varies, but around 2000 cases are reported each year to CDC. Although RMSF cases have been reported throughout most of the contiguous United States, five states (North Carolina, Oklahoma, Arkansas, Tennessee, and Missouri) account for over 60% of RMSF cases. The disease is most prevalent in the South and Midwest with the highest rates reported in southeastern North Carolina and southwestern Oklahoma (Figure 25.7). The disease is more prevalent in the spring and summer months but has been reported throughout the year in the United States.
FIGURE 25.7 Map showing the number of spotted fever rickettsiosis cases by county in the United States in 2012. In the United States, the majority of cases of spotted fever rickettsiosis are attributed to infection with Rickettsia rickettsii, the causative agent of Rocky Mountain spotted fever (RMSF), but might also be from other agents such as Rickettsia parkeri and Rickettsia species 364D. RMSF is ubiquitous across the United States, which represents the widespread nature of the three tick vectors known to transmit RMSF: Dermacentor variabilis in the East, Dermacentor andersoni in the West, and Rhipicephalus sanguineus, recently recognized as a new tick vector in parts of Arizona. Historically, much of the incidence of RMSF has been in the Central Atlantic region and parts of the Midwest; however, endemic transmission of RMSF in Arizona communities has led to a substantial reported incidence rate. .
Source: MMWR 2015; 62(53):92
The incubation period ranges from 2 to 14 days. Onset of symptoms is abrupt with fever, headache, chills, myalgia, and malaise. Frequently this is accompanied by gastrointestinal symptoms of nausea, vomiting, abdominal pain, and diarrhea, which can lead to confusion and delay in the diagnosis. The characteristic rash usually appears 3–5 days after the onset of fever. In many cases it appears first on the ankles and wrist and then becomes generalized. Involvement of the palms and soles is considered characteristic but often appears late in the course of the acute illness. The rash is initially maculopapular and becomes petechial and hemorrhagic as the illness progresses. Vasculitis involving the brain, heart, liver, and kidneys may cause complications from seizures to congestive heart failure and acute renal failure.
Fatality rates have decreased over the years with improvements in early detection and treatment. Risk factors associated with a higher mortality rate include increasing age, delay in initiation of chemotherapy, male gender, and glucose-6-phosphate dehydrogenase deficiency.
Diagnosis
The initial diagnosis of Rocky Mountain spotted fever is largely based upon clinical signs and symptoms including fever, headache, myalgia, rash, and epidemiology (geographic and seasonal variability). Treatment should be initiated before laboratory confirmation of the diagnosis. In endemic regions, an appropriate constellation of symptoms and signs is sufficient justification to begin treatment, even in those with no discernible history of tick bite.
Rickettsia rickettsii infects the endothelial cells that line blood vessels and does not circulate in large numbers in the blood unless the patient has progressed to a very severe phase of infection. For this reason, blood specimens (whole blood, serum) are not always useful for detection of the organism through polymerase chain reaction (PCR) or culture. If the patient has a rash, PCR or immunohistochemical (IHC) staining can be performed on a skin biopsy taken from the rash site. This test can often deliver a rapid result. These tests have good sensitivity (70%) when applied to tissue specimens collected during the acute phase of illness and before antibiotic treatment has been started, but a negative result should not be used to guide treatment decisions.3
Biopsy of a skin lesion obtained with a 3 mm punch biopsy can establish the diagnosis of RMSF. Direct immunofluorescence testing or immunoperoxidase staining can be performed for R. rickettsii on a skin biopsy specimen and may offer a more timely diagnosis if the laboratory is equipped with the appropriate methodology. A skin biopsy has been shown to be approximately 70–90% sensitive.3
The gold standard serologic test for diagnosis of RMSF is the indirect immunofluorescence assay (IFA) with R. rickettsii antigen, performed on two paired serum samples to demonstrate a significant (fourfold) rise in antibody titers. The first sample should be taken as early in the disease as possible, preferably in the first week of symptoms, and the second sample should be taken 2–4 weeks later. In most RMSF cases, the first IgG IFA titer is typically low or negative, and the second typically shows a significant (fourfold) increase in IgG antibody levels. IgM antibodies usually rise at the same time as IgG near the end of the first week of illness and remain elevated for months or even years. IgM antibodies are less specific than IgG antibodies and more likely to result in a false positive. Physicians requesting IgM serologic titers should also request a concurrent IgG titer.3
Treatment
Rocky Mountain spotted fever responds to treatment with doxycycline. Starting treatment early in the course of the disease before the rash is apparent is critical in reducing mortality and morbidity. Patients should be treated for at least 3 days after the fever subsides and until there is evidence of clinical improvement. The standard duration of treatment is 7–14 days. Doxycycline or another tetracycline is considered the drug of choice, but chloramphenicol is preferred during pregnancy because of tetracycline’s effects on fetal bones and teeth.4
Medical surveillance
It is essential that laboratories working with R. rickettsii have an effective system for reporting febrile illness in laboratory personnel. A medical surveillance program should include evaluation of potential cases and, when indicated, institution of appropriate antibiotic therapy.
Prevention
At present there is no commercially available vaccine for Rocky Mountain spotted fever. The best means of prevention remains avoidance of contact with ticks, wearing protective clothing, and using insect repellents. Body checks with particular attention to the scalp, pubic, and axillary hair should be conducted daily for at-risk workers. Ticks can be removed using forceps and gentle traction, being careful to remove all of the mouth parts from the skin. Tick bites should be cleansed and care taken during removal to prevent crushing the tick and contaminating fingers with tick tissue and feces that is potentially infectious. In endemic areas, physicians caring for injured and ill workers should be periodically reminded of the importance of early diagnosis and treatment to prevent serious sequelae. In the laboratory, biosafety level 2 (BSL2) practices, containment equipment, and facilities are recommended for all nonpropagative laboratory procedures including serological and fluorescent antibody tests and staining of impression smears. Biosafety level 3 (BSL3) practices and facilities are recommended for all other manipulations of known or potentially infectious materials, including necropsy of experimentally infected animals and trituration of their tissues, and inoculation, incubation, and harvesting of embryonated eggs or tissue cultures.5
References
- 1. Johnson JE, Kadull PJ. Rocky Mountain spotted fever acquired in a laboratory. N Engl J Med 1967; 227:842–847.
- 2. Walker DH. Rickettsia rickettsii and other spotted fever group Rickettsiae (Rocky Mountain spotted fever and other spotted fevers). In: Mandell GL, Bennett JE, Dolin R, (eds). Mandell, Douglas, and Bennett’s principles and practice of infectious diseases, 7th edn., 2010:2499–2508. Philadelphia: Churchill Livingstone.
- 3. Centers for Disease Control and Prevention. Rocky Mountain spotted fever. http://www.cdc.gov/rmsf/symptoms/index.html (accessed June 17, 2016).
- 4. Chapman AS, Backend JS, Folk SM, et al. Diagnosis and management of tickborne rickettsial diseases: rocky mountain spotted fever, ehrlichioses, and anaplasmosis—United States: a practical guide for physicians and other health-care and public health professionals. MMWR Recomm Rep 2006; 55(RR-4):1–27. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5504a1.htm (accessed on July 2, 2016).
- 5. Chosewood LC, Wilson DE, Centers for Disease Control and Prevention, National Institutes of Health. Biosafety in microbiological and biomedical laboratories, 5th edn. HHS publication no. (CDC) 21-1112, 2009. Washington, DC: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institutes of Health. Available at: http://www.cdc.gov/biosafety/publications/bmbl5/ (accessed on July 2, 2016).